From the Rich and Powerful to the Poor and Dignified
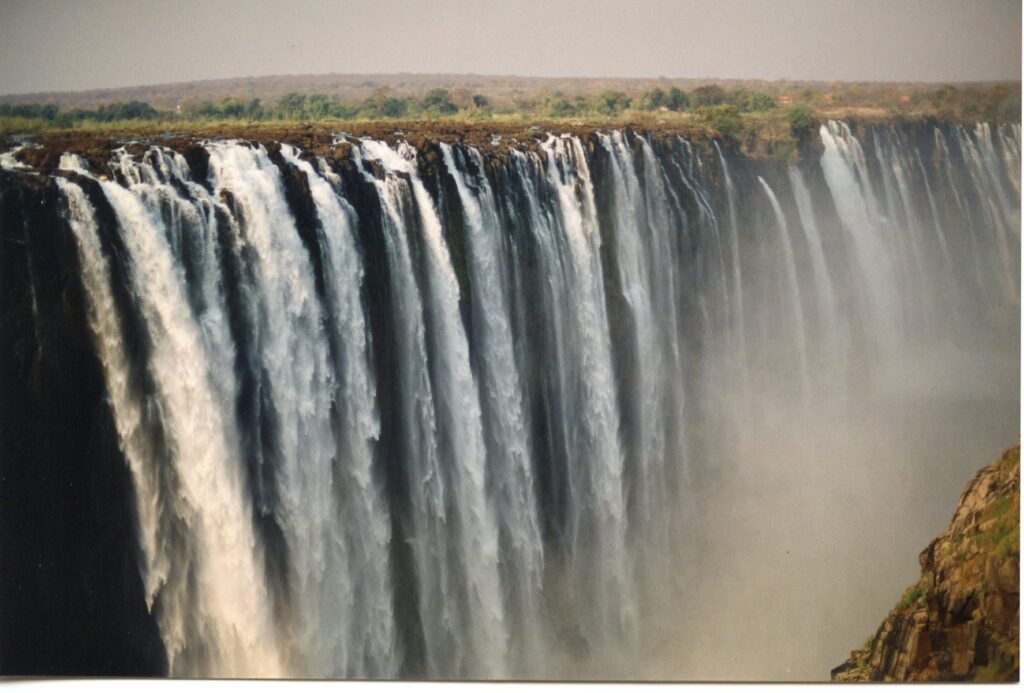
The weather is cool and breezy in Bulawayo, the second largest city in Zimbabwe. It’s a city with wide streets, wrought-iron architecture that might remind you of New Orleans, flowering trees and fresh, breezy air. It is also a city with characteristic long queues for the bank and the gas stations, with people foraging for bread and foreign exchange. Zimbabwe is a tough place in which to get by.
We started our trip just yesterday but it seems much longer than that. While waiting in the lobby of the former-Sheraton-now-Rainbow Towers hotel for our ride to Bulawayo, hotel staff began literally rolling out the red carpets. As we quickly assessed, the president of the country was soon to arrive. That would be Robert Mugabe, reviled by western countries as an arrogant and deluded dictator, and here, sardonically referred to as “Bob.” How to describe him? Think Enron. There has been no natural disaster in Zimbabwe, no civil or cross-border wars, no Communist rebels; so why the severe economic downturn? Why is it people cannot even find bread to buy? Why is it that people cannot even access their own money out of their own bank accounts? Why have Dunlop Tires and Hertz, among many other corporations, pulled out of this country? Disastrous government policies that penalize its people, who are hard working, long suffering and much too diplomatic and kind. So in strode Mugabe and his retinue, along with the president of Senegal. I snapped a photo of “Bob,” now immortalized in my scrapbook, and someday immortalized in the history books alongside others of his kind. 
Just to give you an idea of how difficult it is to manage in Zim, look at what we had to do to get transport to Bulawayo. Though we had reservations with Air Zimbabwe, their computers had been down for two days. Unable to call to get through, Peter Dhlamini, my host, friend and one of the founders of the ZHA, visited their offices several times, but the lines were long with other travelers, all trying to get tickets. Eventually, we lost our reservations and tried to hire a car. Well, without Hertz, we only had Avis, which had no cars. Peter finally located a friend, “Luckey,” who had a car, and Peter, Collen Zhuwao, the general secretary of ZHA, Luckey and I started on our long journey, in pelting rain, through the Zimbabwe countryside.
But today more than made up for any inconveniences. We started our day by visiting Andrew, owner of a tool shop, and his 18-month old son Michael, who has hemophilia. Imagine having a baby with hemophilia and not having any access to a hematologist or factor! So far so good for them, but as Michael grows, bleeds may increase in frequency. We discussed dosing, factor brands, symptoms and what to expect as Michael grows older. I gave Andrew a copy of Raising a Child With Hemophilia and urged him to read it as Michael develops. Michael had not yet been registered by the ZHA, so we recorded all the information they would need to add him to the registry.
We next visited the Bulawayo branch of the ZHA, located at Mpilo Hospital, and met Ndemba, a young man with hemophilia who mans the office. The clean and tidy office is in need of a computer, printer and refrigerator for factor donations. We also met the CEO of the hospital, and Phineas, the Matron, an energetic man and registered nurse who handles all the hemophilia cases. The reason for this is that–try to comprehend this–there is no hematologist in Bulawayo. None to service the 18 registered patients. Things are so bad in Zimbabwe that there is a “brain drain,” with all the professionals and skilled people fleeing the country. Yet the hospital itself is clean and operational, settled in a quiet area, surrounded by beautiful trees and tropical plants.
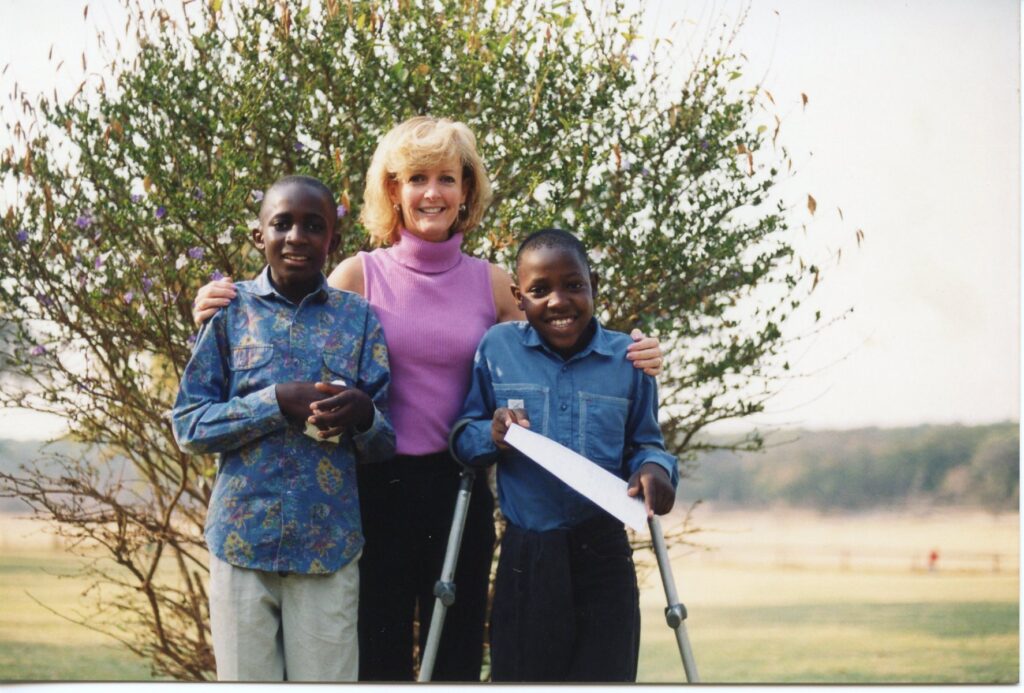
Last visit of the day was to the home of one child who made a permanent impact on my life: Khumbs. I first met Khumbs on my 2000 visit. A motherless child, he had just had his leg amputated the year before when a knee bleed had not resolved (pooled blood eventually can lead to gangrene). He was only nine years old. I saw him again in 2001 at our first camp in Zimbabwe. Shy, sweet, he followed me around the camp, propelled by his crutches, wanting to communicate though he could not speak English. Smiling was our language. Next year, his father died. Left an orphan, he was faced with living with his grandmother, who lived in a rural village. Living in rural Zimbabwe and having hemophilia could be a death sentence. But his uncle stepped in and adopted both him and his brother, who also has hemophilia. Now both boys are living with their uncle, who also has three other children, and both attend school and look strong and healthy.
As we pulled up to their house, I waved enthusiastically to Khumbs and he waved back. I was so happy to see him again! His framed picture hangs on my office wall and I had never once forgotten him in all the years. He and his brother had grown so tall that I was dwarfed; their uncle has cared for them remarkably well. We had brought with us reporters from the local TV and newspaper and we filmed the reunion, and interviewed with them. Our story will appear on the news in the coming weeks.
I pledged to put both Khumbs and his brother in our program Save One Life, so they can begin receiving sponsorship money. Their uncle only earns the equivalent of $20 US a month as a librarian. He must pay money for transportation to his job, which consumes most of his income. I don’t know how they manage; I really don’t. Save One Life will effectively double his salary, and give the family the money they need to get the boys to Mpilo for treatment when needed. We enjoyed sitting in their yard, playing with Khumbs’ toddler nieces and gaining renewed respect for the very desperate lives of the poor. Somehow, in the midst of chronic pain, poverty, economic collapse, a pompous government and repeated loss, this hemophilia family has managed to keep its dignity and hope.
(Photos: Andrew, baby Michael and Laurie; Bulawayo’s stunning architecture; Getting by selling vegetables; Khumbs and his brother)