Hemophilia is a genetic bleeding disorder that prevents blood from forming an effective clot. Without an effective clot, bleeding from injuries may be prolonged or not stop. This can cause joint damage or other complications, and may be life-threatening.
Hemophilia is rare: it’s estimated that only about 20,000 people in the United States have hemophilia. Hemophilia A occurs in approximately 1 in 5,000 male births. Hemophilia B occurs in about 1 in 20,000 male births.To put this in perspective, Down syndrome occurs in 1 of every 700 births, and spina bifida occurs in 1 to 2 of every 1,000 births.
- Vasoconstriction. Muscles in the damaged blood vessel wall tighten, narrowing its diameter and reducing blood flow inside the injured vessel. Even in people with hemophilia, vasoconstriction in blood vessels may sometimes be enough to stop blood flow from small cuts.
- Platelet plug. Platelets are activated at the site of the injury, causing them to become sticky and adhere to the wound and to each other. The sticky platelets plug the hole in the blood vessel.
- Fibrin clot. The platelet plug is weak. To prevent it from breaking down and falling out, restarting the bleeding, the plug must be strengthened and held in place. This is done with fibrin, a tough fibrous substance produced by a complex reaction of plasma proteins called clotting factors. Clotting factors travel in the bloodstream.

 When anyone is cut, they bleed. People with hemophilia also bleed, although they do not “gush” blood, as is commonly believed. They are not in any greater danger of bleeding to death than anyone else. If the cut is shallow, as from a paper cut or a small razor blade cut while shaving, pressure can be applied to the wound. Pressure – placing your hand firmly on the bleeding to stop the flow of blood – pinches the blood vessel wall to close off the tear. If the cut is large or deep, special medicine might have to be given to stop the bleeding.
When anyone is cut, they bleed. People with hemophilia also bleed, although they do not “gush” blood, as is commonly believed. They are not in any greater danger of bleeding to death than anyone else. If the cut is shallow, as from a paper cut or a small razor blade cut while shaving, pressure can be applied to the wound. Pressure – placing your hand firmly on the bleeding to stop the flow of blood – pinches the blood vessel wall to close off the tear. If the cut is large or deep, special medicine might have to be given to stop the bleeding.
People bleed all the time. Sometimes they don’t even realize it. You may have bumped your leg today, and you may have broken some blood vessels. Your broken blood vessels may have healed so quickly that you did not even get a bruise.
But if you have hemophilia, the bleeding may have continued at a slow and steady rate until a large “black and blue” mark developed. This may take hours. Bruising may just be bleeding under the skin. Usually this is nothing to worry about.
Some people with hemophilia have no working factor in their blood. Others with hemophilia have some working factor but not enough to stop all bleeds. Some people bleed every week, some every month, others maybe only once a year. How often a person with hemophilia bleeds depends on how much factor works in the blood. Severe hemophilia means little or no factor works in the blood. Medically it is described as less than 1% active. People with severe hemophilia tend to bleed often, sometimes once or twice a week, even with no known injury! Severe hemophilia is hardly ever fatal, however, in countries like the United States.
Moderate hemophilia means some factor works in the blood. Medically, we say between 1-4% is active. Bleeding occurs usually only after some injury, and maybe only once a month on average.
Mild hemophilia means a lot of factor works in the blood. Medically, we say 5-25% active. Bleeding sometimes doesn’t happen even after an injury. Bleeding occurs maybe only a few times a year. People with mild hemophilia need to have factor when having their teeth pulled or when having surgery.
People with severe hemophilia are known to have spontaneous bleed, bleeds that seem to have no cause. Sometimes their factor levels are so low that just normal everyday activities, like walking, running or doing chores, can cause a bleed. Spontaneous bleeds usually occur in places of the body where there is a lot of activity and stress, particularly the joints. Ankles are common sites for bleeds, because ankles bear so much of the body’s weight and absorb shocks.
People with hemophilia can have different types of hemophilia depending on which factor does not work in their blood. There are at least 13 factors in the blood. Any one of them may not work properly in someone with hemophilia. This is important to know, because different types of hemophilia require different medicines.
In most people with hemophilia, factor VIII is missing or does not work correctly. This is known as factor VIII deficiency or hemophilia A. Factor IX deficiency is the second most common type of hemophilia. This hemophilia is also known as hemophilia B, or “Christmas” disease.
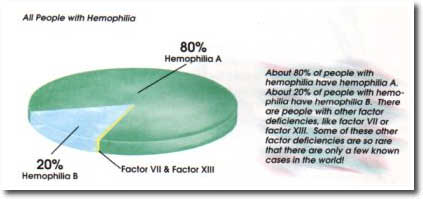
About 80% of people with hemophilia have hemophilia A. About 20% of people with hemophilia have hemophilia B. There are people with other factor deficiencies, like factor VIl or factor XIII. Some of these other factor deficiencies are so rare that there are only a few known cases in the world.
Currently, there is no cure for hemophilia. But scientists are always trying to find a cure. They believe the answer lies in gene therapy. The chemical directions for blood clotting are found on a certain gene in each cell of the body. When you have hemophilia, the directions are scrambled, and the body can’t read them correctly. The body can’t produce enough factor that works.
To cure hemophilia, scientists hope to repair or replace the faulty gene. This could mean taking genes with the correct directions for making factor and inserting them into the cells of a person with hemophilia. Scientists believe the new gene will give the correct directions to the body to start producing high levels of factor. The person with hemophilia might now develop successful blood clotting.
Yes. Unless they find a cure, you will always have it. Some people think of hemophilia like other diseases that get better or worse, but hemophilia is more like having a finger or toe that never worked correctly from birth. The body can’t fight hemophilia like other diseases, because there is nothing to fight! Hemophilia is not a germ or infection. A protein in my blood does not work properly. Everything else works successfully in my blood and body.
It is rare, but yes! If a man with hemophilia married a woman who was a carrier then they might have a girl with hemophilia. The chances of having a girl with hemophilia would be 50%.
There are girls with hemophilia, and boys with hemophilia, whose mothers are not even carriers! Occasionally something goes wrong inside the cells of a developing baby, even when the parents have nothing wrong with them. In one-third of all cases of hemophilia, the mother is not a carrier of hemophilia! Something just went a little wrong inside the baby.
- Vasoconstriction. Muscles in the damaged blood vessel wall tighten, narrowing its diameter and reducing blood flow inside the injured vessel. Even in people with hemophilia, vasoconstriction in blood vessels may sometimes be enough to stop blood flow from small cuts.
- Platelet plug. Platelets are activated at the site of the injury, causing them to become sticky and adhere to the wound and to each other. The sticky platelets plug the hole in the blood vessel.
- Fibrin clot. The platelet plug is weak. To prevent it from breaking down and falling out, restarting the bleeding, the plug must be strengthened and held in place. This is done with fibrin, a tough fibrous substance produced by a complex reaction of plasma proteins called clotting factors. Clotting factors travel in the bloodstream.
Hemophilia means that the fibrin net does not get made properly. Without the fibrin net, the platelet plug falls out and bleeding continues.
Why does this happen? With hemophilia, one of the 13 clotting factors does not work properly. When a blood vessel is torn, usually the blood vessel constricts and the platelets make a plug. The clotting factors start giving each other directions: factor III, for example, directs factor VII. But then something doesn’t work right – the directions for blood clotting. The creation of the fibrin net stops and the bleeding continues.
Anyone can start bleeding internally following a blow to the abdomen, head, arm or leg, or after a fall that injures the knee or elbow. People without hemophilia may stop bleeding and heal on their own. People with hemophilia may continue to bleed internally, slowly and steadily, sometimes for hours or even days after the injury. They may not even realize they are bleeding at first. But it is necessary to get medicine immediately. Why?
Let’s look at an example. A joint is a place where two bones meet. Inside the joint is a space called the joint cavity. This cavity allows you to move the two bones. The bone ends that meet to form the joint are protected by a smooth substance called cartilage, which covers the end of each bone like a cap.
 Now let’s imagine that someone with hemophilia falls and injures a knee. Blood steadily leaks into the joint cavity. The joint begins to swell and ache. The joint becomes stiff. The leg cannot bend, and walking becomes difficult and painful. Even worse, blood has substances in it called enzymes. Enzymes break down other substances. As blood accumulates in the joint cavity, enzymes begin to break down the blood to get it out of the joint where it does not belong, to be reabsorbed into the body. This is good. But as the enzymes do this, they also start to break down the cartilage covering the bone ends. If joint bleeds are allowed to continue for too long or happen too many times, the cartilage may become permanently rough and jagged, making smooth joint movement painful.
Now let’s imagine that someone with hemophilia falls and injures a knee. Blood steadily leaks into the joint cavity. The joint begins to swell and ache. The joint becomes stiff. The leg cannot bend, and walking becomes difficult and painful. Even worse, blood has substances in it called enzymes. Enzymes break down other substances. As blood accumulates in the joint cavity, enzymes begin to break down the blood to get it out of the joint where it does not belong, to be reabsorbed into the body. This is good. But as the enzymes do this, they also start to break down the cartilage covering the bone ends. If joint bleeds are allowed to continue for too long or happen too many times, the cartilage may become permanently rough and jagged, making smooth joint movement painful.
Muscles are also a common spot for internal bleeds. Muscles can act like sponges, and can hold a lot of blood. Muscle bleeds cause swelling and can limit movement. Luckily, there are plenty of symptoms when someone gets a joint or muscle bleed: many say these bleeds feel “tingly,” “funny” or “hot.” Medicine (or clotting factor) can help stop a bleed before there is damage to the muscle.
People with hemophilia can lead practically normal lives by using commercial prescription medicine, called factor. This medicine, injected into the veins, replaces the factor that does not work properly. With all the factors working properly, the directions for blood clotting are passed along until the fibrin net is formed.
 Factor comes in small bottles and looks like packed white powder. When properly mixed with sterile water, factor is ready to be infused – injected directly into a vein. When it is infused, factor does not go directly to the site of the bleed; it takes a trip around the body. All veins carry blood back to the heart, so factor goes back to the heart, too. Then the heart pumps factor out to all parts of the body at the same time, including the place that is bleeding. Factor can work quickly to stop a bleed.
Factor comes in small bottles and looks like packed white powder. When properly mixed with sterile water, factor is ready to be infused – injected directly into a vein. When it is infused, factor does not go directly to the site of the bleed; it takes a trip around the body. All veins carry blood back to the heart, so factor goes back to the heart, too. Then the heart pumps factor out to all parts of the body at the same time, including the place that is bleeding. Factor can work quickly to stop a bleed.
 Infants and small children with hemophilia are usually infused by doctors and nurses who are experts in hemophilia care. As a child grows older, he can be infused at home by his parents, who are trained by the doctors and nurses. Eventually the child with hemophilia can learn to infuse himself. An infusion doesn’t take long and can be done at home, at school or at work. It’s great to be able to self-infuse because a person with hemophilia can go almost anywhere and do many activities knowing that the factor he carries will help stop a bleed quickly.
Infants and small children with hemophilia are usually infused by doctors and nurses who are experts in hemophilia care. As a child grows older, he can be infused at home by his parents, who are trained by the doctors and nurses. Eventually the child with hemophilia can learn to infuse himself. An infusion doesn’t take long and can be done at home, at school or at work. It’s great to be able to self-infuse because a person with hemophilia can go almost anywhere and do many activities knowing that the factor he carries will help stop a bleed quickly.
Your eye color, hair color and texture, skin color and many of your facial features – including the shape of your nose – are physical characteristics inherited from your parents. As you grew into a baby inside your mother, you were created with special cells from your father and cells from your mother. These cells had chemical “directions” in them that told your body exactly how to develop into a baby. Because some of these cells were from your father, his directions might have told you to have blue eyes like him. Or, because some of the cells were from your mother, you might have received directions to have the same curly hair as she, not the straight hair of your father. The possible combinations of the characteristics you can inherit are endless!
Guess what else can be inherited? Diseases and physical disorders. Hemophilia is a disorder that can be inherited. It can be inherited from the mother.
 A mother who can pass hemophilia along to her baby is called a carrier. This means that inside her cells she carries directions for blood clotting that are scrambled, although her blood knows how to clot correctly. When her baby inherits the cells with the scrambled directions, the baby’s body cannot “read” the directions and his blood cannot clot. This is known as hemophilia.
A mother who can pass hemophilia along to her baby is called a carrier. This means that inside her cells she carries directions for blood clotting that are scrambled, although her blood knows how to clot correctly. When her baby inherits the cells with the scrambled directions, the baby’s body cannot “read” the directions and his blood cannot clot. This is known as hemophilia.
If the mother who is a carrier had several baby boys, it’s possible that some might not have hemophilia. Sometimes the scrambled directions are passed along; sometimes they are not. Each time the mother is pregnant with a son, it is like a flip of a coin: heads, she has a boy with hemophilia; tails, she does not. Each flip of a coin has a 50% chance of coming up heads or tails.If the mother is a carrier and the father does not have hemophilia, their daughters have a 50% chance of being a carrier. They will not have hemophilia, but they may have children with hemophilia.
When a person inherits hemophilia, he receives directions for blood clotting that are mixed up chemically. His body cannot read them, and cannot clot blood properly.
Your body is made up of trillions of individual cells. A cell is like a living building block; the smallest unit of living tissue. All human life starts as a single cell inside the mother. From the moment that the egg from the mother joined with the sperm from the father to create a new life, it was already determined that the one resulting cell would grow to be a boy or girl with or without hemophilia.
How could one cell determine all this? The answer lies in your genes. Inside that one cell are all the chemical instructions needed to direct the cell to make copies of itself and then divide in two. By dividing in two repeatedly, the cell reproduces itself until there are millions, then trillions of cells. Genes direct how all the copying and dividing will be done. Genes direct some cells to become heart cells, others to grow to be brain cells, and still others to grow to be teeth, the stomach lining, or your fingernails. Genes also direct your bodily functions: how your heart will work; perhaps how quickly you will be able to learn, or run; how your blood will clot.
 The genes of some children do not have the correct directions for blood clotting. Children with hemophilia inherit these genes from their parents. Why do some children in a family inherit these genes, yet their brothers or sisters sometimes don’t?
The genes of some children do not have the correct directions for blood clotting. Children with hemophilia inherit these genes from their parents. Why do some children in a family inherit these genes, yet their brothers or sisters sometimes don’t?
The answer to this question lies in the chromosomes. The genes are wrapped into 23 pairs of chromosomes, found in every single cell in your body. On one pair of chromosomes only lies the gene with the incorrect directions for blood clotting, which causes hemophilia. It lies on the same chromosomes used to determine if you will be a boy or a girl. These are called the sex chromosomes. This is why hemophilia is “sex linked” and why usually only boys get hemophilia. Follow closely now!
Inside the mother’s egg are 23 chromosomes, or half of the mother’s genetic characteristics. Inside the father’s sperm are 23 chromosomes, half of the father’s genetic characteristics. When the egg and sperm are joined, they give the new cell 46 chromosomes, arranged in 23 pairs, exactly what is needed to begin growth from a cell to a baby.
 Will this new life be a boy or a girl? The last pair of the 23 pairs will determine this. Under a microscope, the sex chromosomes of a girl look like “XX.” The sex chromosomes of a boy look like “XY.” Whether it’s a boy or a girl, you see that there is always at least one X chromosome present. The mother’s egg always carries an X chromosome. But the father’s sperm can carry either an X or a Y chromosome. When the egg and sperm meet and begin a new life, the egg already has an X, but the sperm may give an X to make a girl or a Y to make a boy. It is the father who always determines the sex of the baby!
Will this new life be a boy or a girl? The last pair of the 23 pairs will determine this. Under a microscope, the sex chromosomes of a girl look like “XX.” The sex chromosomes of a boy look like “XY.” Whether it’s a boy or a girl, you see that there is always at least one X chromosome present. The mother’s egg always carries an X chromosome. But the father’s sperm can carry either an X or a Y chromosome. When the egg and sperm meet and begin a new life, the egg already has an X, but the sperm may give an X to make a girl or a Y to make a boy. It is the father who always determines the sex of the baby!
 Although the father’s chromosomes determine the sex of the baby, the mother’s chromosomes determine whether the baby will have hemophilia. The gene with the scrambled directions for blood clotting (hemophilia) is found only on the X chromosome. If the mother is a carrier of hemophilia, then half of all her X chromosomes have on them the scrambled instructions for blood clotting. The other half has clear directions for blood clotting. The clear directions, even if they are only on half her chromosomes, are enough to allow the mother to have normal blood clotting. This is why she does not have hemophilia.
Although the father’s chromosomes determine the sex of the baby, the mother’s chromosomes determine whether the baby will have hemophilia. The gene with the scrambled directions for blood clotting (hemophilia) is found only on the X chromosome. If the mother is a carrier of hemophilia, then half of all her X chromosomes have on them the scrambled instructions for blood clotting. The other half has clear directions for blood clotting. The clear directions, even if they are only on half her chromosomes, are enough to allow the mother to have normal blood clotting. This is why she does not have hemophilia.
But she is a carrier, so her son might receive from her the X chromosome with the scrambled directions. This is why a mother who is a carrier has a 50% chance of having a son with hemophilia. She might donate an egg with either an X chromosome affected by hemophilia or one not affected by hemophilia. This is also why her daughter might be born a carrier. The daughter might receive an affected X from her mother, but an unaffected X from her father (whose X chromosomes are all unaffected). She would not have hemophilia because the X chromosome from her father would still contain the clear directions for blood clotting.
When a boy with hemophilia, who has an affected X chromosome, grows up and has children, he will give either his X or his Y chromosome to each of his children and will determine their sex. If he gives an X chromosome to create a girl, it will have to be the one with scrambled directions for blood clotting, because, having hemophilia, all of his X chromosomes are affected. All his daughters will be carriers.
