When it’s a new year, we tend to make goals, lists, things we want to accomplish. I love doing this myself, and I love bringing other’s goals to fruition. That’s pretty much our aim at Save One Life, to assess needs, meet needs, and offer people with bleeding disorders who
live in the most difficult of circumstances hope and even a new beginning.
I recall meeting Jitendra, age 14, in India in November 2012. I met a group of mothers and fathers and their children on the trip in Bhubaneswar, in Orissa, one of the poorest states in India. It is rich in history though, with so many ancient temples, deemed World Heritage sites.
Though I met many families that day, one truly stood out. A father with a driven, intense, haunted look in his eyes. We enrolled his son, Jitendra, and I asked the father his story: what had happened to them, what was the greatest challenge they faced? Usually we hear that there is no factor, they have little money, the child misses school. This father’s
story was different.
He was living in a tent with Jitendra, as a homeless person, as floods had washed away their home. (And by home, I mean probably a thatched roof hut. They live 150 kilometers away from the hospital. The father works on a farm, and must travel far away form his only son each day.
I was stirred by the intense look on his face; his eyes seemed to bore into me.
When I asked him what one thing would
make your life easier, expecting him to say free factor, he said emphatically and without hesitation: a vegetable selling business, to open a roadside
vendorship, to be near his son. Awesome
answer. Needs 50,000 rupees ($1,000) to start. That is an enormous amount of money for him, about one year’s salary.
Can you imagine if someone gave you one year’s salary, and you were homeless? The temptation is always there to drink, have fun, squander it. Not this guy. He used the money Save One Life gave him from its Micro-Enterprise Grant program to open the stand, and earn his own living. Now he is near his son and doesn’t have to be away on the farm working. What a Happy new year for him!
And even better? The Orissa government, one of the poorest in India, is buying factor. Not a miracle, but the result of intense lobbying by the hemophilia chapter there and its leadership—a young man
with hemophilia named Chitta.
If they can achieve those new year goals, imagine what we here in the US can do!
Visit www.saveonelife.net to learn how you can help the poor with hemophilia!
Character cannot be developed in ease and quiet. Only through experience of trial and suffering can the soul be strengthened, ambition inspired, and success achieved. —Helen Keller
Helen Keller’s quotation could be a the tagline for Advocacy 101, a class I feel I attended this weekend. I received a text Friday morning from my brother Tim, telling me our 82-year-old mother had been admitted to the hospital in the early morning hours. Apparently she had fallen in the night and couldn’t get up–yes, just like the commercial says.
When I finally arrived in Springfield, I went straight to the hospital observation ward. My mother was very ill, that was clear. The doctors were running tests on her to rule out arterial blockage, stroke or neurological issues. Her main symptom was extreme vertigo, as she had no balance at all, which left her exhausted and nauseated, and shaking. She had not been able to eat all day. Fortunately, when I left her three hours later for the evening, she was perking up and looking and feeling better. The doctors were very helpful, and explained everything they could, in the best way they could. The nursing staff was excellent and we felt she was getting top-notch care.
As I left, I realized I had not been in a hospital, in a medical situation, in a very long time, probably more than four years ago, when my son was last admitted with me around (appendicitis). My advocacy skills were a bit rusty.
Well, the great care she received Friday was from the day staff. The next day I returned with my sister-in-law Lee, and my mother looked like she was suffering, having had an ordeal through the night, including a 3 am MRI. She was curled up on one side, unable to lift her head, nauseated to the extreme. She had not had anything to eat or drink in forever. She said the noise from the admin desk (just a few feet away) from the “girls” at the desk was loud, obnoxious, keeping her tense and unable to rest. She rang and rang the call button, but no one came to assist her. She listed all her frustrations.
Lee poked her head out of the curtain that barely screened her from the rest of the ward and ordered, “She needs a room, now. She is very uncomfortable.” And this lead to, when are we getting the room? Do you know, within 15 minutes they had a room for her. They gave her a pill for nausea, changed her, wheeled her upstairs and brought her delicious broth to drink. My mom felt better within 30 minutes. She sat up and ate the soup.
Lee also discovered that the nurse did not have it noted on her charts that my mother is diabetic: staff should really not be giving her muffins with high glucose content! Noted. And her diet was changed.
I was proud of my sister-in-law for being there, and for so immediately requesting an improvement. That’s true advocacy in action. It was a reminder of everything I learned 27 years ago when my son with hemophilia was born: how to politely make my medical rights known, to make my needs known, to speak up for a baby who cannot speak for himself. And not to back down when you know you are right. These skills weakened over time when not used; I was slower to advocate for my mother than my sister-in-law was!
I just learned that she has been discharged; so we will arrange to have her brought home, just in time for Christmas. And from where did I first learn medical advocacy? It wasn’t really hemophilia; it was from mom of course. As one of seven children, I watched her handle hospitals and doctors many times with my active brothers. And I saw her get action when she spoke up. The nurse mentioned to me that my mother is refusing a script for a walker, which we all wanted her to have. That’s advocacy and pride. That’s my mom, my first advocacy teacher.
Interesting Book I Just Read
Metallica This Monster Lives: The Inside Story of Some Kind of Monster [Kindle]
Joe Berlinger and Greg MilnerA story about the making of a documentary of one of the most successful metal bands, which was going through a crisis that threatened to destroy itself. In 2001 Metallica was reeling from losing its bass player, yet had to produce a new album, its first in years. The film team that produced two excellent documentaries, Brother’s Keeper and Paradise Lost (and the widely panned Blair Witch Project 2), now documented the band composing, fighting and enduring therapy with a performance coach. 1600 hours of footage turned into a feature documentary, and entered the Sundance Festival. But the book–an oddity. More about the filmaker and his career. Berlinger is too close to his subjects to be objective, and at times, revels giddily in his chumminess with Lars, the drummer. But I enjoyed it, even if it is an unevenly told story; Berlinger comes across as a very nice person, sincerely trying to do his best as the game plan keeps changing radically. Lars does not come across well. Fans may cringe at hearing these thrash metal superstars bare their feelings towards each other. A great book for psychotherapists or filmakers in training. The Kindle version is riff with missing periods at the end of sentences. Two/five stars.
A natural phenomenon occurred October 7-8: a Blood Moon with an accompanying lunar eclipse. I’m interested in how and why this term, which is
becoming more widespread, developed, and in all things related to blood. The origin of the term is religious, according to Christian pastor John Hagee.
From the internet I gleaned this: Hagee used the term “blood moon” to apply to the full moons of the ongoing tetrad – four successive total lunar eclipses, with no partial lunar eclipses in between, each of which is separated from the other by six lunar months (six full moons) – in 2014 and 2015. John Hagee appears to have popularized the term in his 2013 bookFour Blood Moons: Something is About to Change.
Hagee speaks of a lunar tetrad as representing a fulfillment of Biblical prophecy. After all, the moon is supposed to turn blood red before the end times. Why are more and more people are using the term “blood moon” to describe the four full moons of a lunar tetrad? No one really knows!
But in astronomy, writers often describe a totally eclipsed moon as appearing “blood red.” A moon may look
red during a total lunar eclipse because of sunlight that is filtered and refracted by Earth’s atmosphere. From the website
“earthsky.org”:
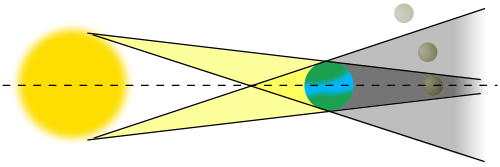
“During a lunar eclipse, you’ll see the Earth’s shadow creeping across the moon’s face. The shadow will appear dark, like a bite taken out of a cookie, until the shadow completely covers the moon. Then, during the breathtaking time of totality, the
shadow on the moon’s face often suddenly changes. Instead of dark, it appears red. Why?
“The reason stems from the air we breathe. During a total lunar eclipse, the Earth lies directly between the sun and the moon, causing the Earth to cast its shadow on the moon. If Earth didn’t have an atmosphere, then, when the moon was entirely within Earth’s shadow, the moon would appear black and invisible.
“Thanks to Earth’s atmosphere, what actually happens is much more subtle and beautiful. Earth’s atmosphere extends about 50 miles (80 kilometers) above Earth’s surface. During a total lunar eclipse, when the moon is submerged in Earth’s shadow, there is
circular ring around Earth – the ring of our atmosphere – through which the sun’s rays pass.
“Sunlight is composed of a range of frequencies. As sunlight passes through our atmosphere, the green to
violet portion of the light spectrum is, essentially, filtered out. This same effect, by the way, is what makes our sky blue during the day. Meanwhile, the reddish portion of the spectrum is least affected.
“What’s more, when this reddish light first entered the atmosphere, it was bent (refracted) toward the Earth’s surface. It’s bent again when it exits on the other side of Earth. This double bending sends the reddish light onto the moon during a total lunar
eclipse. Depending on the conditions of our atmosphere at the time of the eclipse (dust, humidity, temperature and so on can all make a difference), the surviving light will illuminate the moon with a color that ranges from copper-colored to deep red.”
So, watch for the “blood moon” during a lunar eclipse!
Great Book I Just Read
Three Dog Nightmare
Chuck Negron
My first LP was “Golden Biscuits” in the 1970s, and so began my life-long love of Three Dog Night, the popular rock band of the 1960s and 70s. Who knew
the debauchery and drug-induced devastation that took place? Negron, lead
singer with a powerful voice, details his rise to stardom and then the slow and sharp decline into
the life of a junkie. He spends his entire fortune on heroin, destroys
relationships and the band, and brings his children into the world addicted to
meth and heroin. That he is still alive and performing is a miracle, after
being so near death for so many years. He engages in crime, sinks to the level
of street junkies, gangs, and would do anything—anything—to get his next fix.
It is a shocking and disturbing portrait of the high price of fame and a
natural inclination to addiction. I finished this in two nights: hard to put
down and technically an easy read. I deeply applaud Negron for sharing his life
and how he turned it around eventually. Hard to understand are his complaints and
character assassinations about his bandmates, particularly Cory Wells, which come
across as juvenile and unappreciative. Negron should never judge anyone after what he inflicted on others. Still, I will always love Three Dog Night! Negron is still touring solo, and Danny and Cory are touring as TDN. Three/five stars.
I’m attending the World Federation of Hemophilia Congress in Melbourne, Australia. I’ve been attending these since 1996, when it seemed I knew everyone, and now, with 4,000 attending from 128
countries, it’s at once hard to see familiar faces, and yet, that’s a positive side effect of the success of the WFH’s outreach to so many patients, physicians and partner organizations globally.
Aung from Myanmar: The face of
hemophilia in the Third World
The opening plenary yesterday, led by WFH president Alain Weill, welcomed everyone, and provided some surprises.
My concern is always access to product for those in developing countries. Indeed, in the opening ceremony Sunday night, Weill announced something to the effect that this was a great time in hemophilia, a great era. Treatment for all! That’s the slogan. Well, yes and no. Not if you’re a child in the heart of Africa.
But there was great news at the plenary Monday morning. Weill said that since 1996 WFH has distributed 248 million IUs of product in 86 countries, helping about 90,000 people with bleeding disorders. (I’m proud to note that Project SHARE, a program run by two people, me and Zoraida, has distributed since 2002 about 60 million IU to about 55 countries) Weill announced some amazing product donation pledges: Biogen Idec and Sobi have agreed to donate 500 million IUs of factor over the next five years to WFH’s Humanitarian Aid Program. Grifols committed to 60 million IUs over a three-year period. And the Italian Centro Nazionale Sangue (CNS) announced donations of up to 30 million IUs of factor VIII per year over a five-year period.
As the Soci CEO said, we want to stop thinking of donating product at the end of the day, and make it the first thing we think about in the morning. In other words, this will allow WFH to plan strategically how to use product donations to improve care, rather than leaving it to act in crisis mode (which is often how Project SHARE operates, and it’s difficult to operate like that). So the donations will be charity used with a strategic purpose to enhance development. Awesome.
Alain Weill and Dr. Gabriele from CNS Italy
I attended an interesting meeting called the Management of Hemophilia with No or Limited CFCs, withCarlos Gaitan Fitch of Mexico as facilitator.
Four speakers presented how they manage hemophilia with little or no factor.
Ricarte Felipe, new president of HAPLOS of the Philippines, age 50, reviewed his life growing up without factor. He spoke from a wheelchair that day, and from which he was confined for 3-7 years of his young life. He was diagnosed at age 8 with hemophilia A. At age 12 lost his left eyesight in an accident. Yet he managed to get a college diploma despite the challenges. Only in 1986 was he started to be infused with plasma and cryo. In 1988
he received his first infusion of factor due to a tooth extraction. What a survivor!
He shared that factor in the Philippines is $100 for a 300 IU vial. And while in 2010-2013, he was treated mostly with CFC (clotting factor concentrate), factor is not available much in the Philippines. The government does not buy it. And it is so expensive, most families cannot afford it.
So how do Filipinos manage? Support from HAPLOS consists of psychosocial workshops, camps, workshops, and “Mass healing,” where attendees at church pray for the patients.
What was sadly missing from this touching account was this: what is HAPLOS doing to secure factor, to change the destiny of the children being born right now with hemophilia in the Philippines? It’s difficult to listen to the suffering, especially from a leader, and not hear about what is that organization going to do to change this.
Dr. Gilian Wharfe, University of West Indies, Jamaica, also presented. I’ve known Dr. Wharfe for many years and have visited Jamaica twice
to meet with her and the patients. She clearly laid out the issues facing Jamaica: high unemployment, stagnant economy, inflation, and factor costing $50 per unit, beyond what parents can pay (we know; they contact us regularly), makes it impossible for the government to consider putting factor in the federal budget. The only access to factor is from donations.
Laurie Kelley with long time friends Massod Fareed Malik and Deon York, each presidents of their country’s hemophilia organizaiton (Pakistan, New Zealand)
With approximately 200 patients, and only one HTC at UHWI (which is not a public hospital; the patients must pay), one national blood
transfusion center and several collection centers, Jamaica struggles to provide care to hemophilia patients. The stopgap measures for care include: prevention of bleeds, early treatment of bleeds (How can you do that with limited access to factor, distances to travel, long waits for cryo or FFP to be thawed, etc?) and educating patients about how to avoid bleeds and recognize bleeds early.
It was a rather bleak assessment, and a classic example of life in the developing world with hemophilia. You have to admire the physicians like Dr.
Wharfe who must practice under these conditions.
Dr. Daniel Hart,hematologist at Barts and The London School of Medicine, spoke about his experiences twinning with Bangladesh and The Royal London Hospital Haemophilia Centre. It was an excellent summary about how twinning can help slowly transform a country. Twinning means the medical center in a developed country pairs with one in a developing to share best practices and hopefully, to help resource the less developed center.
Aussies Steve Russell and Fred Wensing help Aung of Myanmar to attend the Congress and buy a wheelchair to take home
Dr. Hart described how Bangladesh uses “.001 IU per capita,” compared to 5.8 IU per capita in Australia. Numbers like these give hard, cold facts to global factor disparity. He covered a lot of ground in his talk, but what stuck out were two things:
1. Diagnostic accuracy is fundamental, as well as access to expertise, advocacy (really important—hitting up the government, emergency
centers, pushing the national hemophilia standards everywhere), and patient and physician education.
2. Perspective: Hart showed an old trailer in an old photo, and said this was how the treatment center in London, now a world class center,
started. In just an old trailer. His photos progressed to a high-end sports car!
So conditions now do not have to persist over time. Treatment can improve. But… and the Philippines should heed this… you cannot get anywhere if
you don’t fix up the trailer. Advocacy is a must—pushing the national agenda, having a strategy, and first knowing what you want.
I changed plans for my blog tonight after burning out from too much computer work to go to a matinee movie. What to choose from? I could easily recommend Captain Phillips or Rush… both excellent. But I chose Ender’s Game, not expecting too much. It’s received 62% on the “Tomatometer,” not exactly stellar (no pun intended).
Here’s the plot, which I shamelessly rip off (with added commentary and at least one grammatical correction) from RottenTomatoes.com:
“In the near future, a hostile alien race (called the Formics, [kind of like a hybrid giant praying mantis/”Alien” critter]) has attacked Earth. If not for the legendary heroics of International Fleet Commander Mazer Rackham (Ben Kingsley) [who has now disappeared, presumed dead, and who is a Maori from New Zealand], all would have been lost. In preparation for the [presumed] next attack, the highly esteemed Colonel Hyrum Graff (Harrison Ford) and the International Military are training only the best young children to find the future Mazer. [Why children? Because their minds integrate and process computer simulations faster than adults…]
Ender Wiggin, a shy, but strategically brilliant boy is pulled out of his school to join the elite. Arriving at Battle School, Ender quickly and easily masters increasingly difficult war games, distinguishing himself and winning respect amongst his peers. Ender is soon ordained by Graff as the military’s next great hope, resulting in his promotion to Command School. Once there, he’s trained by Mazer Rackham, himself [who–surprise!—is not dead], to lead his fellow soldiers into an epic battle that will determine the future of Earth and save the human race. Based on the best-selling, award winning novel, ENDER’S GAME is an epic adventure…”
I thought this was going to be a purely sci-fi, CGI, blow up the aliens tale, but it’s much more than that. It does proceed slowly with the plot, focusing on character development. The real action doesn’t take place until the very end. It’s gotten its share of criticism for a variety of reasons, but… I liked it!
I liked that it’s about children applying themselves, finding value in their studies, discovering a higher calling. It’s a movie about leadership and youth; what does it take to be a “leader”?
A variety of youth leaders are portrayed, from different genders to nationality and races: Ender’s own sister, talented like him in her own right, was deemed “too compassionate.” Another leader, short and muscular, was too aggressive and demeaning, authoritative. You wonder about Ender himself—yes, he’s smart, but can he get people to follow him? Over the course of the movie, you watch how he develops his own leadership style, and matures into a true leader, demonstrating strategy, psychology, risk-taking, challenging the status quo [his elder leaders], accepting responsibility when things go wrong, and most of all, honoring his own values. These are all important ingredients to making an effective leader. He embodies all three styles of leadership: positional, situational and transformational. For that alone, the movie should be seen.
Especially by hemophilia youths. We’ve been hearing for a long time that we are victims of our own success. When you have aliens threatening the earth (or HIV threatening the blood supply) you can more easily mobilize an army to do battle—and leaders arise from the masses to spearhead change. When things are cool, good, life is chillin’, it’s harder to get people to train, study and implement leadership for when things don’t turn out right in the future. During a crisis is not the time to study leadership for the first time. we’re victims of our own success; we no longer have an alien to fight, or do we?
Healthcare reimbursement maybe? Could be. Those of us educating and fighting for access to therapies, and lowered copays are not the ones who will be needing this in the future; it’s our kids. They are the ones, the “Enders” we need to enlist now. Teach them how to do battle in the Battle Room while we still have our own Rackhams (starring Michelle Rice maybe?) with us? Something to think about.
In any case, bring your child to see this movie, and talk about leadership afterwards. There is a lovely twist at the end that brings it all together as a feel-good movie. Ask:
What traits make for effective leadership? Is it a popularity contest? What hurts about being a leadership? What do you stand to lose? To gain? Who are your child’s admired leaders? If they are stuck on sports stars, broaden their vision of who and what a leader can be. And let him or her know that the hemophilia community has its leaders too… who will one day need the youth to come forward, like Ender, to plot new courses in our universe, to protect our community from invaders, both pathogenic and economic.
HemaBlog Archives
Categories
LA Kelley Communications - You are leaving our site
You have clicked on one of our advertiser’s links. Our provision of a link to
any other website or location is for your convenience and does not signify
our endorsement of such other website or location or its contents.
Would you like to continue?
Download Now
Would you like to be added to our email list to continue to recieve future editions of PEN in PDF format?
 I recall meeting Jitendra, age 14, in India in November 2012. I met a group of mothers and fathers and their children on the trip in Bhubaneswar, in Orissa, one of the poorest states in India. It is rich in history though, with so many ancient temples, deemed World Heritage sites.
I recall meeting Jitendra, age 14, in India in November 2012. I met a group of mothers and fathers and their children on the trip in Bhubaneswar, in Orissa, one of the poorest states in India. It is rich in history though, with so many ancient temples, deemed World Heritage sites.
 He was living in a tent with Jitendra, as a homeless person, as floods had washed away their home. (And by home, I mean probably a thatched roof hut. They live 150 kilometers away from the hospital. The father works on a farm, and must travel far away form his only son each day.
He was living in a tent with Jitendra, as a homeless person, as floods had washed away their home. (And by home, I mean probably a thatched roof hut. They live 150 kilometers away from the hospital. The father works on a farm, and must travel far away form his only son each day.