As World Hemophilia Day was celebrated in many countries, I chose to spend this year’s WHD in Kenya, a country I have been visiting since 1999. The nonprofit I founded, Save One Life, has three programs here—microgrants, scholarships and sponsorships—each touching directly the lives of many children and young men
with hemophilia.
The day was organized by the eloquent Dr. Kibet Shikuku, a hematologist at the Kenyatta National Hospital in Nairobi, and James Kago, a young man with hemophilia. Dr. Kibet welcomed about 70 family members—parents and children with hemophilia or von Willebrand disease. The day provided an overview of hemophilia for the press members present, the needs of
Kenya, and words of wisdom for moving forward from this day.
“My prayer today,” Dr. Kibet invoked, “is that we walk forward as a group, so we can advance the issues that affect us. We are one body with different endowed parts. We want to be worthy partners for better hemophilia care in Kenya.”
One main goal is to ensure better diagnosis, he added. With a population of 43 million, Kenya should have roughly 3,000- 4,000 with hemophilia. About 400 patients were identified at one point (meaning they came in at one time in their lives for treatment), but the numbers are not reliable. Only about 50 patients are regular visitors to the treatment center.
Other take aways from Dr. Kibet: “We Kenyans we have every right to be provided for by things that affect us with hemophilia. We must take charge of our own destiny. Togetherness will make us strong. Speak with one voice! We must lobby the government to support testing and availability of factor. Time to speak out and speak up about hemophilia: our community, our accomplishments, our needs.
Speak Out, Create Change was the slogan for World Hemophilia Day, the April 17 event that commemorates the birthday of World Federation of Hemophilia founder Frank Schnabel, an American who envisioned our global community working together to improve care.
Speak out… for kids like Emmanuel
Kibet thanked the WFH and Project SHARE for their support of donated factor. He also
thanked donors in US, especially those who support Eldoret project, like the
Indiana hemophilia treatment center and Novo Nordisk Haemophilia Foundation.
He also thanked the Jose Memorial Haemophilia Society and showed a photo of a man
who was in bed for four days with a severe bleed. The JMHS provided him with a donation
of factor.
He noted that there is simply not enough factor; once Kenya secures enough
regularly, then it can offer home therapy.
This is a huge point. Kenya is large, and roads can be difficult. Most patients
living in rural villages have no way to get to the treatment center in Nairobi,
the capital, or can afford transportation. I know first-hand as I have
traversed these roads quite a few times. Imagine taking a public bus, crowded,
hot, hours long, with a painful psoas bleed or worse.
Emmanuel
James Kago
The audience really responded to this idea and asked about home therapy… hoping that someday, someday speaking out… will create change.
Kenya has come a long way, and I was very excited to see at this meeting more change is afoot, all for the best, to create the kind of unity and one voice Dr. Kibet mentioned.
The informative meeting was concluded and a delicious lunch served outside on the hospital grounds. I was able to hang out with a few of the boys I’ve known for years and years: Jovan, Peter, Charles (who has a baby now!), Emmanuel, John.
Lucy Kago asks a questionMrs. Mwangi and StephenMoline Odwar and Laurie KelleyJohn with Laurie Kelley
Simon, Laurie Kelley, PeterLaurie Kelley with Lucy and son SimonPeter, Maureen Miruka, Jovan Odwar
Today was a field trip, outside of the bustling, clogged streets of Nairobi. We headed to Murang’a, a town about 90 minutes away, off on the highways pitted with deep and numerous potholes. The shoulders of the highways are crumbling and soft so in dodging the potholes, we have to be careful not to veer too close to the shoulders or we will need up in a ditch.
You may think Africa is hot (the very name means “Away from the cold”—A frika), but Kenya is quite pleasant, with cool breezes, mostly dry air, and even chilly in the evening. No wonder so any settlers came here and stayed. The climate, the rich red soil, the friendly people make Kenya a country where people dream of living.
Maureen Miruka, mother of two-year-old Ethan and founder of the Jose Memorial Hemophilia Society, was our fearless driver. With us also was Paul, the 24-year-old administrator of the Society. How nice that Maureen hired him—he has hemophilia and many of the young men with hemophilia cannot hold down jobs. Remember that there is no factor in Kenya unless it is donated, and the donations are only enough for a few.
Our first stop was the Murang’a District Hospital, where we met the gracious Senior Nursing Officer Danny Mengai. Joining us later was Dr. Nguyo. Maureen had met them previously, explained about hemophilia and this time brought with her their very first ever donation of factor! This is factor that my organization Project SHARE had donated to her organization. This was the kind of teamwork and outreach I like to see. Imagine: Murang’a has a higher than normal concentration of people with hemophilia and there has never till now been any factor in the hospital. And you can bet that fresh frozen plasma is hard to come by as donating blood is not a tradition in Kenya, or in any African country.
I learned today that a big teaching opportunity for the JMHS would come in December: this is when the vast majority of circumcisions are done. Why? I asked. For religious purposes? No, Maureen replied: school holidays. Boys are circumcised around age 12 and this is when we can get referrals for bleeding disorders to the Society. Dr. Nguyo assured us he would check with Maureen at that time, and also refer anyone suspected of a bleeding disorder.
Back in the Toyota and then on to visit patients. This was our very first official field visit—sorry, the second. We must give Paul credit. He had visited previously by himself to do the groundwork, and take down patient information for Save One Life. And he did an excellent job! Our goal is to start enrolling patients from Kenya, and ask anyone reading this blog to consider sponsoring a child form Kenya. The needs are terribly great and it won’t take much to change their lives.
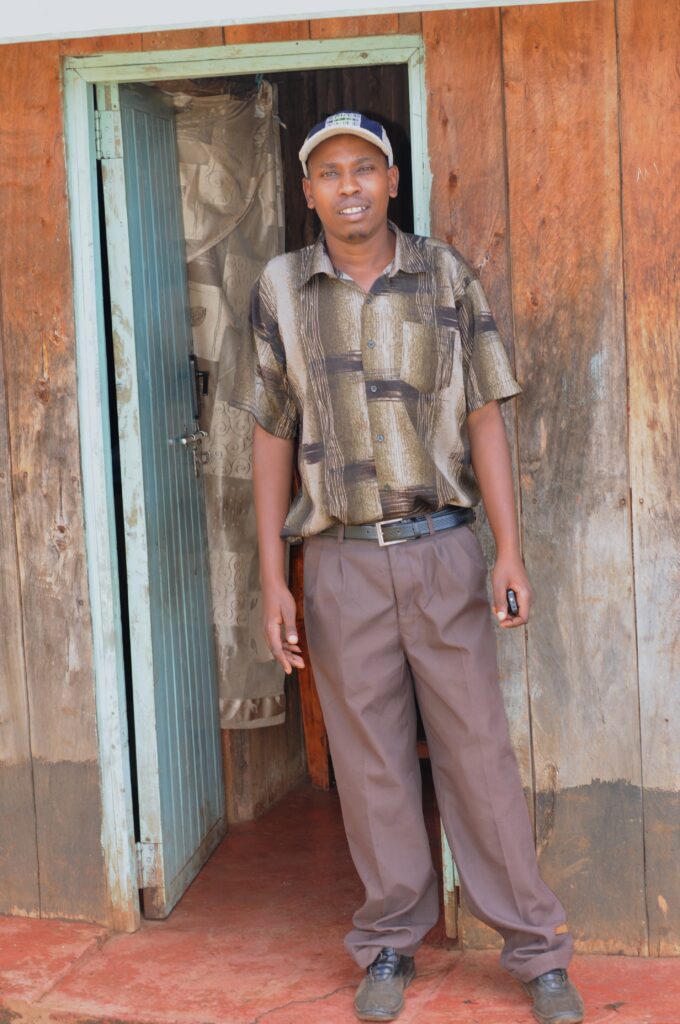
Take Peter for example. Just down the street from the hospital, on a red dirt road, in a small apartment lives Peter, age 19, with hemophilia. He is thin and speaks softly, like most Kenyan boys. He was so curious about his condition, and wants to be a doctor when he grows up, “So I can help other people like me. Because I know how they suffer.”
That’s an understatement. I am not sure we can understand how much these children suffer, with no relief, night after long and desperate night. (Photos: Peter; his kitchen; Me with family)
Let’s imagine what it is like for Peter when he has a bleed. There’s no money to get to the hospital. He has no crutches, of course, no wheelchair. He remains housebound. He tries to hide it from his distraught mother. She is single, and caring for Peter, and his brother, who has emotional problems as well as hemophilia, and also has adopted her two nieces, abandoned by her sister. The mother makes only about $20 US a month washing clothes and housekeeping for people. Peter’s bleed worsens, as does his pain. At night they all sleep in one room (the only other room they have, which also functions as a “kitchen,” because it has a charcoal pot in it) probably a few of them crammed into one bed. If anyone moves, this sends shooting, excruciating pain from the bleeding joint. Peter can’t get up and watch TV as a distraction, or Facebook, or do Wii, or pop a painkiller, or grab ice from the freezer or treat himself to a Coke. They don’t have a refrigerator, and own nothing but the basics—a table, chairs, couch, a bed or two, a boom box. If he gets up he’ll wake everyone. And in Africa, kids don’t whine and demand and complain. They suck it up with dignity. He lies there all night, trying to control the pain. The last thing he wants is for his mother to find out, which will add to her worry and suffering. He learns to be stoic and fight the pain, because there is simply no other choice. This bleed goes on day after day and night after night. It finally subsides… until next week, when this scenario happens all over again.
This is his life, and he cannot imagine any other.
We record his family history, ask him about his schooling, and his plans. We learn that his brother is in a mental ward. The entire family was terrorized last year during the post election violence. Thugs entered their home, set it ablaze, and chased them out into the streets. This is a nice, Christian, impoverished family, with two young men with hemophilia; they deserve nothing of what has happened to them. The younger brother, already fragile, is suffering from post-traumatic stress disorder. We make plans to go visit him. He’s ready to come home, but the family has incurred $350 in fees and like most developing country hospitals, the patient is not released until the bill is paid. You hear that right. Peter’s brother could be there indefinitely. We’ll see about that.
Who wouldn’t want to sponsor Peter? What a lovely young man; so sensitive and sweet, so gracious and kind. If he were placed in America, there would probably be nothing he couldn’t accomplish with his winning perspective.
The road calls, and we soon leave, after first handing out some presents to the family. On to the next patient: Peter’s uncle, also named Peter. He is older, with a family: wife and two children. He lives, well, basically, in a jungle. We park by the side of the road, surrounded by banana plants, overgrowth, trees and vines. Someone actually lives in that thicket of vegetation. We pull over under a big tree and a crowd of children gather, from the other side of the street. They giggle and whisper, “Mzungu!” and cover their mouths. What does that mean, I ask Maureen. Maureen smiles and says, “White.” Not many people like me make it out here, I guess.
I dissolve our differences by hauling out my stash of Tootsie Pops. Never, ever travel in developing countries without them. They withstand the heat and luggage manhandling, and are beloved by everyone. I hand out one to each bystander and immediately have fans!
We should have brought machetes because to get to Peter the uncle, we have to step over rocks and push back the big banana leaves. A short walk down the twisty sort-of trail and we arrive at their plot of land. Such poverty.
A split-log home, tin roof, muddy ground. The floor inside the house is missing; it’s just mud. There is no electricity. There are indicators of various levels of poverty and this is one key: do they have electricity? Believe it or not, you can do without plumbing. An outhouse will do and most people in the villages have them. But when you don’t have electricity…. You might as well be living in the 1800s. No, even earlier, in this case.
This family owns nothing, nothing. No vehicle, hardly any furniture. A homemade chicken coop housed a few chickens that had no food or water and the heat was growing. I felt for them, sadly. They cackled unrelentingly. A dog was penned in the back, also in a homemade kennel, with hardly any ventilation, whining to be released. The children padded around barefoot, the wife was a bit cautious, not too friendly. (Photos: the outhouse; Peter with family)
I gave the children the customary Tootsie Pops, which they eagerly accepted, and a superball and a toy kitten that shook when you pulled his tail. They were frightened by the toy at first. Then they thought it hysterical, and they made it shake over and over. I had rescued some toys from the CVS store which operates right beneath my office. Apparently, they ditch whatever they don’t sell every month: perfectly good toys, baby items and medical items. I retrieved toys for kids, baby strollers, thermometers, heat wraps, you name it. Yeah, I am a Dumpster Diver and proud of it. Everything is neatly wrapped in clear plastic bags and in perfect, new condition. And these kids had a ball with the toys.
After our interviews with Peter, we headed for the next house. Also perched in a jungle-terrain, on a hill, Charles’s home at least has electricity. And the animals look well cared for. We were greeted by the father, Sampson, an elegant elder man, his wife, who eyed us warily, and later told us this was the first time she ever met anyone else who had a child with hemophilia (! She must be about 60), Charles and his new wife, Hannah.
Charles approached us on a crutch, with obvious crippled joints. But what a nice young man: age 24, speaking fluent English (Kiswahili is the national language but most educated people—meaning grammar school and high school—can speak English as Kenya was once an English colony). Charles shared so much with us: his hopes to return to college and study electrical engineering, because he has a knack to fix anything, and he longs to contribute to his family. His parents are elderly. How much longer can they work and support him? It’s such a source of shame for an African man to be supported by his own parents. Hannah was sweet and gave me a little tour of their farm. The animals were all housed in self-made, split-log cages, but really well done and humane. A cow, goats, chickens and a dog. As clean as can be for living in jungle-like surroundings. They don’t have a refrigerator and Charles could really use one for ice for his joints. He lives so far from any hospital and they of course don’t own any kind of transportation! Not even a horse.
We were so impressed with the family. So good, high hopes, willing to work hard. Charles needed $350 to get his school fees paid for so he can return and get his degree. He just doesn’t have that kind of money. People like him, Peter and all the others we met live day to day. It’s truly survival. And when thugs burn your house down, or the rains come and wash away your farm or crops, you are really threatened with starvation and just pure survival.
We just cannot imagine their daily lives. I have a hard time, and I have seen it in front of me. How do they do it?
And yet I never hear a complaint, or curse. The only think I hear are blessings: May God bless us for our work, may we have a safe journey, thank you for helping us. Now maybe you can see why I return over and over. Despite their poverty, they have a richness many of us in developed societies lack.
We parted on such happy terms, and we all chattered on the way back about what a diamond in the rough Charles was! Peter too, in a different way.
We visited two more families, Stanley, a grown man, and Derrick, a one year old and actually Paul’s nephew. By then it was really growing late and I was out of Tootsie Pops and just about anything else in my purse that I had given away.
Our last stop of the day was at a home of a better off family. They have a proper concrete home, electricity, and the father is employed as a teacher. The son with hemophilia neatly dressed with shoes. We had a nice courtesy visit, and afterwards, to show their appreciation, the mother presented Maureen with a magnificent rooster!
They popped the rooster into a plastic bag, tied the top and carried it out to the car, its crested head popping out. When they opened the “boot” (trunk), the animal lover in me sprung out. We just can’t put a rooster all trussed up in a plastic bag into a hot trunk! It was 90 degrees and we had a two-hour journey back on horribly bumpy roads! The poor thing…
So I rode with the rooster in my lap, all the way back to Nairobi for two hours at night, petting it as if it were a cat. The doorman at the Holiday Inn was pretty surprised when he opened my door to let me out!
I’d call it a successful day all around for Save One Life and Save One Rooster.
(Please consider sponsoring one of the families mentioned above! Just $20 a month. See http://www.SaveOneLife.net)
Today we met a very special person with hemophilia, who touched us deeply, and reminded us of why we do the crazy things we so—like driving about three hours outside of Nairobi, deep into the Kenyan countryside just to meet one patient. Well, this is why we call our nonprofit “Save One Life.” It’s all about one person at a time.
You cannot separate Simon’s story from the logistics. Sure, he has hemophilia, as does his brother. He’s 26. His wife left him, and he now lives on his mother’s farm. He has the usual untreated bleeds, and hobbles about on crippled legs. We wanted to meet him because we knew he lived in difficult circumstances. Total rural living; you might say primitive, if you judged him by the average American standards.
We headed out at 8 am with Maureen Miruka, founder of the Jose Memorial Hemophilia Society, driving. With us were Paul, a 21-year-old with hemophilia, impeccably dressed as always, and Jeff, our videographer. They picked me up at the Holiday Inn, and off we went.
Over two hours of driving on a highway, dodging the worst potholes you can imagine. The shoulders of the road drop swiftly, so we have to be careful not to veer off. It was like a high-speed obstacle course! Left, right, fast, slow, then the random speed bump. The speed bumps (or “sleeping policemen”) are not marked, and so blend in with the road, and can cause severe damage. The ride seemed to take a lot longer than two hours.
We took a short break to see the breathtaking Rift Valley, 3,600 miles long, and an important source of fossils.
We arrived in Nyahururu, far north of Nairobi, a bustling town. As always, the Kenyans are dressed well, and walking, walking, walking. It seems that everyone walks in this country. I was surprised to see a long line of young men with motorcycles, just waiting. This was local transport, and in a minute I would find out why.
We spotted Simon under a gas station sign, waiting for us. I gave up my front seat when I saw how painfully and slowly he was walking, to give him more room and excluded room. Simon would show us how to get to his home.
We turned the corner to Simon’s street. The street is a dirt road off the main road. The red, rich soil of Kenya covers every inch of this long road. Up we went, as the road ascended and we dodged not potholes, but regular bikes with massive loads of grass or wood, their drives pushing them resolutely upwards. Or women and children carrying huge loads of potatoes in sacks, supported by bands around their heads. Or cows, stumbling down the road into town.
We spun in the soil, which was muddy at times, and began to wonder how on earth Simon could manage this. We finally arrived at his farm, perched high on a hilltop with a spectacular view of Kenya. To get to his farm you must climb up another dirt pathway strewn with rocks.
The logistics of getting him help for a bleed are mindboggling. When Simon gets a bleed, this is what happens:
Simon, in pain, has to either walk down the dirt path to the dirt road, then walk over three miles on this dirt road, down the hill and into town. Then he has to wait for the local bus to drive him to Nairobi, to the only hospitals that know how to care for people with hemophilia. Our drive took over two hours, and that was going fast. On a bus, you can expect to take two to three times longer as it makes stops, and goes slower.
All the time, Simon is in great pain.
We arrived probably with our mouths gaping: the farm is rustic but pretty and what a view! His mother greeted us, but wasn’t smiling, the way Kenyans usually are when they smile. Indeed, the entire family was grim, and tight-lipped. “They are stressed,” Maureen said to me aside.
We sat inside the small home (we would call this a shed) where his mother lives. I glanced around and noticed the corrugated tin roof (nothing new there; this is a given in the developing world) and cardboard. The walls were split logs, and the “wallpaper,” or covering, was cardboard, through which the light peeped in.
We chatted with Simon a long while, recording his family history and discussing his bleeding pattern. This would give us the necessary information to register him with Save One Life and find him a sponsor. Jeff also gave him an interview, and Simon spoke in Kiswahili, the national language, as his English is very limited. He shared his frustration, not at hemophilia, but of the incredibly long distances he must cover just to get some kind of help.
It was clear to us all that Simon needed to keep factor at home. To my delight I learned that he had been taught to self-infuse. But the government of Kenya buys no factor, and so there rarely is any available. Imagine traveling all that way in terrible pain only to arrive at the hospital and be told there is no factor! Or, come back tomorrow for your FFP.
Simon’s mother surprised us with a wonderful home cooked meal: mokimo, a national dish. It was the only meal we would eat all day (and only my second meal in two days!!). Things started to lighten up a bit. We presented Simon with a gift of factor VIII; we shared how Save One Life would provide funds for transportation. And we pledged somehow we’d keep him stocked with factor. By the time we shuffled back to the car, everyone was beaming, like a little ray of light brightening his future.
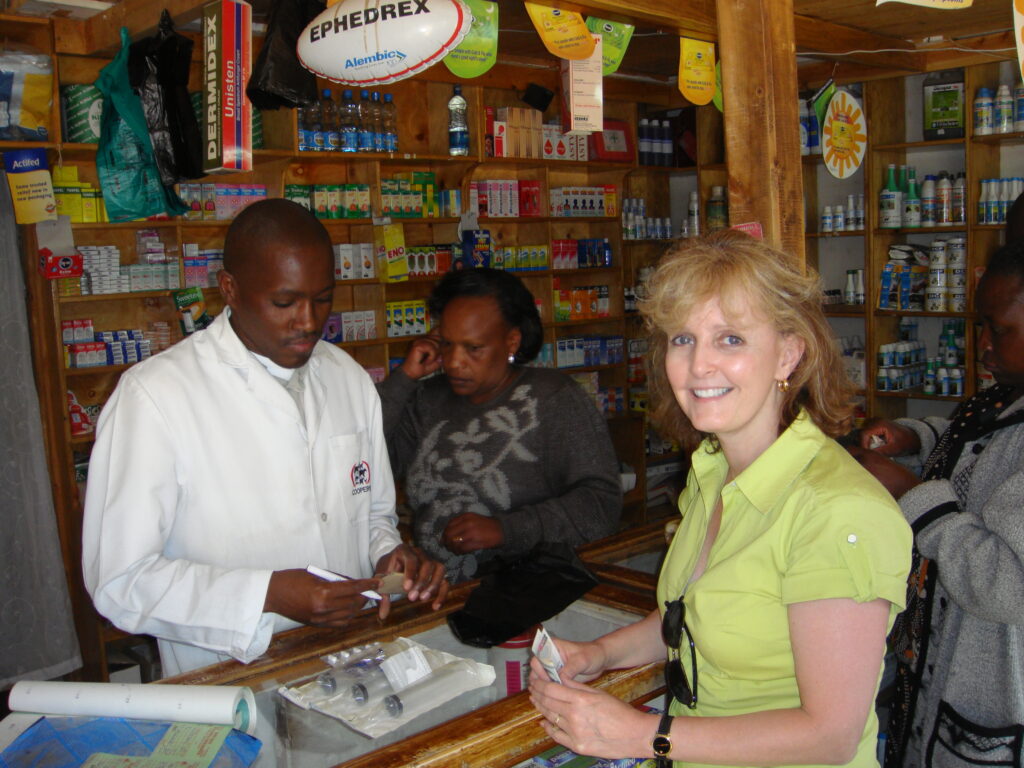
Before we left, we stopped at the local pharmacy where I bought Simon syringes, needles and medical tape. Things we so take for granted are not free here! And some cash so Simon could ride one of those taxi-motorbikes back up the hill to his home.
The ride back was both sobering and exciting. We had defined ways to help this very special man.
Our day was far from done. The ride back—three hours again—was only to plan what to do about another young man, age 21, hemophilia A, in a mental institution. He was placed there following the post-election violence that engulfed Nairobi last fall. This young man’s home was invaded, ransacked and then burned to the ground by electrified hoodlums, as many homes burned all around. I don’t know his whole story: perhaps he was chased, terrorized. Whatever it was, it left him so traumatized and depressed, he had to be committed. We heard he was able to leave now, following two months of treatment.
The problem? His mother, single, with two boys with hemophilia and two nieces, has to pay $340, a fortune, perhaps more than what she makes in a year. The son would not be released unless this was paid. This is the way it is in developing countries. We actually drove at twilight to go see him. We were allowed into the padlocked Men’s Ward, and the rank smell of human beings unable to care for themselves assaulted us. Lying on cot after cot were young men, about 25, all heavily sedated for the evening. The boy’s mother was with us as we tried to wake he son. He awoke and stared at us blankly, through drugged eyes. He looked so small and helpless on the old, thin cot. My God, I thought. This could have been my 22-year-old.
I made the only decision I possibly could; I gave the money to Paul, and tomorrow (Thursday) he would go with the mother and bring this poor child home, where his family could care for him.
This was a day of pure experience and exploration in the lives of two young men in desperate need. We cannot fix everything or everyone, but our motto at Save One Life is “To save one life is to save the world,” and that works just fine for me.
It’s with great pleasure and joy that I’ve returned to Kenya, in east Africa, to visit the patient groups and the patients I have grown so fond of over the past nine years. I first arrived in 2001, returned again last year and was eager to not wait eight years before returning again!
Kenya is best known nowadays in America for its elite athlete runners (one just won the Boston marathon last week) and as the ancestral home of our president. But it is very important for hemophilia care as its national hospital has become a training center for many in east Africa. There are an estimated 4,000 people with hemophilia in Kenya, and about 400 identified and registered. Yes, there is a long way to go in providing care, but seeing where it has come in nine years, it has been making steady progress.
I landed late last night after a six hours flight to London, an overnight stay and then an eight+ hour flight straight to Kenya. I was greeted by Maureen Miruka and partner Sitawa, parents of Ethan, who has hemophilia. Maureen founded the Jose Memorial Hemophilia Society to help organize patients with bleeding disorders and to provide programs that address their needs. Jose was Maureen’s first son, who died three years ago that same evening.
My first stop today was the Kenyatta University Hospital, to visit with the chief hematologist, Dr. Walter Mwanda, and the Kenya Haemophilia Association. We had a wonderful meeting and it was exciting to get caught up on the many outreach activities planned, and the ideas of their young president, James Kago, who has hemophilia. What devotion: James just became a father for the first time on Saturday, and here he was, attending to affairs of the state! Our meeting, originally a courtesy call, lasted three hours. We all share a deep passion for helping those suffering with hemophilia in Kenya, and it showed in our bubbling over of ideas and concerns and a pledge to help the KHA and all patients. (Photo: Dr. Wanda and KHA)
Next stop: a visit with James’s new baby girl Tiffany! It’s been a long, long time since I have held a newborn and there is perhaps no greater joy.
Next stop was to meet at my hotel with Maureen and James, and also Geoffrey Mosongo, a young man with hemophilia who has established a new program to help young men with hemophilia get scholarships, finish school and find work. Geoffrey rightly recognizes the needs patients have as they mature to find employment. The meeting was to put heads together to find better ways to create results. I was very impressed with the level of respect and compassion each has for the other, and for each other’s organizations.
The meetings went on well into tonight, for we are ten hours ahead of Boston time.
Tomorrow I go off for a field visit about two hours outside of Nairobi, the capital, to meet with patients in their homes. Stay tuned!
The Kenyan Flag: The black stripe represents the African people; the red stands for the blood shed for independence. The green represents Kenya’s natural resources. The thin white stripes symbolize peace and unity. The central emblem is a shield of the indigenous Masai warriors.
Good Book I Just Read Pooling Blood by Cheryl D’Ambrosio
This is the true story about two sisters with bleeding disorders (factor V deficiency), as told by their stepmother. It is absolutely compelling; a beautiful tribute to the story of Cheryl’s fight to keep the girls alive, and educate a medical community often ignorant of girls with bleeding disorders. From the opening scene of a blood smeared bathroom, to the blossoming of the girls socially at camp to a near-death experience while on a vacation, the book is a roller coaster of emotions and learning experiences. I started reading it while on the treadmill; three miles never flew by so fast! The book is a testament to advocacy and persistence, and Cheryl is a gifted storyteller.
The only places where the book falls short is when medical or industry related material is shared. The description on page 114 of Bayer’s Kogenate FS production stoppage is completely wrong; the explanation of volunteer versus paid blood donors is outdated and incomplete. The glossary however is very good. Readers should enjoy the story, learn from Cheryl’s experience and prepare to be very inspired.
I flew into Tanzania today, a quick one-hour flight from Nairobi. I was greeted so warmly, so kindly by the members of the Tanzania Hemophilia Society, who made me feel instantly welcome and part of the family. Richard Minja, founder, and I have been communicating for four years, working to establish the society, and when we met he greeted me with an unabashed hug! We feel as though we have already met; so strong are the ties that bind people who live with bleeding disorders.
En route to LumuruBeautiful Kenya
But first, let me finish telling my tale of Kenya. I wish I could bring you all with me to experience what I experienced: glimmers of hope in patients who were desperate for care, for a solution to some very difficult problem. Overall, Kenya has a great physician and hospital at Kenyatta Hospital, but the problems faced by Kenyans with hemophilia are institutional, cultural and logistical. Overcrowded emergency rooms mean that patients wait hours before being seen: those with serious bleeds risk life itself. Factor often is not available, and what little there might be must be used sparingly. The medical staff devote their entire lives to helping patients but even they cannot overcome a culture in which patients are meek, do not speak up when they are bleeding, and do not challenge the current system. The traffic in Nairobi pretty much dictates everything; your entire day is planned around how best to avoid traffic. You can literally sit for hours, inching along. Patients can never get to a hospital quickly this way. So many patients live very far from the hospital, and many do not own cars. How can they get from a rural house on a long, miles long red muddy road to a highway and then into Nairobi when they have no car and no reliable public transport?
So we know what we must do.
On Thursday, I flew back from Zanzibar, and pretty much just sorted myself out the rest of the day, trying to keep up with email. Maureen and her partner Sitawa picked me up at the airport and we met with Salome and Dolphin, two members of the board of directors, to finish plans for the big charity event they were holding Friday.
Charity’s Home
On Friday, April 24, we started our day early by visiting Mrs. Eva Muchemi, of the Diabetes Management and Information Center. She was wonderful! Diabetes and hemophilia actually have a lot of things in common, as both are chronic disorders. Eva gave us many tips in running a nonprofit and establishing family-based programs for education. One of the coolest things I learned (no pun intended) was how to create a “traditional cooler,” to store insulin or any biological product. Using two tin cans, charcoal (abundant in the developing world), and a rubber ball as a stopper, local artisans can make these insulated cooler cheaply. In that way, patients can store insulin at home!
Next stop, the hotel where the event would take place, to check on preparations. The rich smell of roses filled the air and I can see that Maureen and team pulled out all the stops for this event, which is in memory of Jose, Maureen’s firstborn, who died just shy of his sixth birthday on April 25, 2007. Rather than submerge herself in extended grief, she empowered herself to create this society to ensure that no other child should die of untreated bleeding.
Then, Salome, who is a nurse at Kenyatta and also a mother of a child with hemophilia, and I went to visit Charity, a vivacious mother of three who lives in Lumuru, on the outskirts of Nairobi. As we finally disentangled ourselves from vicious traffic, and patiently endured a police roadside checkpoint, we zoomed along the highway. Immediately the countryside unfolded, and a beautiful Kenya revealed itself. It’s a double-edged sword: along with the lush countryside comes increased poverty, though I have to say that rural poverty is quite different than urban poverty. What you forfeit in modern conveniences, you make up for with clean air, space, and peace. But life is hard there.
I snapped dozens of photos long the way, which will have to wait till I am back in the US, where we have high speed Internet. It takes too long to upload photos. But what photos! Wait till you see them all.
Turning onto a rusty and rock-encrusted dirt road, we bounced and banged our way to Charity’s house. We passed donkey-pulled carts, women balancing immense loads of vegetables or firewood on their heads, and random donkeys grazing on the thick grass. Finally we arrived.
Daniel
Charity is a woman with a dazzling smile and lovely, British-clipped accent. She was so excited to have an American visiting her home-what an honor for her! But it was an honor for me. How often do we get this chance, to share intimately in the life of a struggling soul? Out of the house shyly emerged her children: Patrick, 14, Daniel, 11 (who has severe factor VIII deficiency) and giggling Ann, 5. Another cousin tagged along. Daniel actually looked in good shape, though a bit small for his age, while Patrick is slim and robust, strong. We had a tour of the home, the separate “kitchen,” which is a wooden shed, inside which was a steaming pot of soup. The smoke was really thick inside: directly above the pot was a cord of wood, which was being dried by the smoke. Nearby were vats of water–their household supply. Back out in the bright sun, we went to the rear of the house, where I was surprised to see two cows, which give fresh milk daily, and a cute calf. A small cat followed us about. The kids started to loosen up and we took photos.
Inside, we listened to Charity’s story: Daniel misses a lot of school though he is a good student. Education is absolutely paramount to them, for it ensures a future for the entire family. There’s no such thing as welfare for the elderly. You are cared for by your family or not at all. So you’d better believe these kids get educated. Daniel’s knees show signs of arthropathy, especially in the left knee. Unbelievably, though they have electricity, there is no TV, no washing machine and no refrigerator! Try to imagine no refrigerator, especially for a child with hemophilia. A small one costs $200 and we pledged to source finds for one. The kids smiled broadly when I whispered this might mean keeping the occasional Coca-Cola in the house for special occasions.
Patrick wanted to see photos of my family, and my pets, and when I handed him my iPhone, he wasn’t phased by the technology. He immediately got the hang of its touch, and skimmed through my photos, asking such intelligent questions.
Laurie Kelley with Charity and children
David, the father, came by, limping. He had been mugged two years ago, and left with a shattered leg and has been unable to work. When I broached the subject of their income, I think tears came to his eyes. For a man not to be able to support his family seemed wrong. I looked about the humble abode, seeing how clean and neat the children were, the wonderful food Charity placed on the table for us to eat, and how attentive they were. Charity earns $35 US a month selling vegetables from their small farm out back.
We will enroll them in Save One Life, which will almost double their monthly income. Charity said they need money most for transport to the city for treatment. They almost always will need a taxi or to pay a driver.
As we spoke, I glanced up at the cupboard next to me, on which was an appropriate plaque at eye-level: “Weeping endures through the night, but joy comes in the morning.” Psalm 30:5. So appropriate for a child with savage joint bleeds, and a mother who holds him all night helplessly. To see their smiles today meant we have brought some measure of joy.
When it was time to leave, there were hugs and the kids were all smiles. In fact they piled into the back seat of the car for a lift to homes near the highway, so they could visit a friend. And we returned to the congested city for our big charity event, which I will need to write about in a day or two. Stay tuned!
HemaBlog Archives
Categories
LA Kelley Communications - You are leaving our site
You have clicked on one of our advertiser’s links. Our provision of a link to
any other website or location is for your convenience and does not signify
our endorsement of such other website or location or its contents.
Would you like to continue?
Download Now
Would you like to be added to our email list to continue to recieve future editions of PEN in PDF format?

 The day was organized by the eloquent Dr. Kibet Shikuku, a hematologist at the Kenyatta National Hospital in Nairobi, and James Kago, a young man with hemophilia. Dr. Kibet welcomed about 70 family members—parents and children with hemophilia or von Willebrand disease. The day provided an overview of hemophilia for the press members present, the needs of
The day was organized by the eloquent Dr. Kibet Shikuku, a hematologist at the Kenyatta National Hospital in Nairobi, and James Kago, a young man with hemophilia. Dr. Kibet welcomed about 70 family members—parents and children with hemophilia or von Willebrand disease. The day provided an overview of hemophilia for the press members present, the needs of