Blood, sweat and tears literally flowed at the Dominican “¡Yo Si Puedo!” summer camp in Lomas Linda, Dominican Republic this past week. Blood? Because the 40 children and teens attending all have hemophilia, and when you are exited, attending what may be the brightest spot in your year, running, playing, dancing—oh my, can the Dominicans dance!—and you are never on prophylaxis because there is so little factor available, then you are naturally going to bleed.
No problemo. The good news is that we had plenty of factor for camp, thanks to a generous donation. And you wouldn’t believe how these kids played, knowing they had factor to back them up. With a theme of the “Wild West,” our little cowboys were pretty rowdy!
This is the 11th annual Dominican camp, called “Yes, I Can!” in English. A little over twelve years ago, when I first arrived here, the DR had next to nothing for hemophilia care. No factor, not even donations, a poorly run hemophilia national organization—in name only—and a patient registry of less than 50, if even that. Patients were shut out of participating in their own organization, until one woman and her colleagues decided to shake up the system and return power to the parents. Haydee de Garcia and friends succeeded, and the DR today has a government that buys factor, a patient registry of over 260, regular meetings and events, a strong new organization that is patient-centered, and best of all, a fantastic camp.
Sweat? The humidity hits you like a sledgehammer on this beautiful tropical island nation. My feet swelled within a few hours and I sweated constantly for the next four days. Camp is about 40 minutes outside the capital Santo Domingo, in the rolling hilled countryside. The stunning facility where we hold the camp has stately white houses for dorms, a thatched-roof dining area, a big in ground pool, and no hot water! That’s fine because you look forward to the chilled water to cool you down and wash away the constant perspiration. Three showers a day and back on go the damp clothes, only to be soaked again within an hour in the dripping air.
The acclimated Dominican kids never seem to sweat, though. I watched the in awe as they rolled out of bed at 7 each morning, formed a circle at 7:30 am and did their group calisthenics with “Cuchito” the coach, and then paraded into the outdoor dining area for a hot breakfast. Then there were classes about hemophilia, story times, pool times, a rowdy time with inflatable bouncing castles and jumbo slides and a very special visit yesterday to a rodeo—the first one in the DR! As always, camp ended with a wonderful talent show, including skits about hemophilia, and we were all dancing the merengue when the clock struck midnight.
We had probably the best camp since 1999, when it was founded by Haydee and the Fundacion Apoyo al Hemofilico (FAHEM). Then, it was rustic and without amenities. None of us knew how to run a camp, but still we had a great experience and created fond memories. Fast forward and now we have a world-class camp, and the little boys who attended the first camp in 1999 are now counselors, young men who model everything from how to have manners, to how to be part of a team, how to settle disputes, how to be patient and disciplined, and how to have fun safely.
Tears? That was a surprise for me. I’ve been watching these boys for 11 years, and as a mother, am bursting with pride for the initial campers and the men they have become. Brahian, Javier, Alphonso, Luis, Dámaso, José G., Isaiah, Henry, Carlos and José Luis—what amazing and beautiful young men with hemophilia they all are. When we sat down yesterday morning for a rap session about who they are, what their role is in the future of the organization, leadership, and the importance of them taking on even more leadership in preparation for the day when current leaders are gone, the boys expressed their thoughts and feelings.
It started as a rational discussion about leadership and camp, but then it was as if the past 11 years welled up like a swelling ocean wave, carrying with it all the feelings of little boys who left their mothers for the first time in 1999 to young men who have shouldered silently more pain than most of us know in a lifetime. In giving us, the adults, thanks for what we have done for them—personal sacrifices, long nights of planning, days and weeks of organizing, late night visits to the hospitals–tears began to flow when they realized what their lives may have been like had there been no Haydée, no Mecho, no Dr. Rosa or Dr. Joanne, no FAHEM, no camp. And when one wept spontaneously, several others quietly wept, to release all the common feelings of a decade and in gratitude that their futures have been secured. As one young man said, “These are tears, not from sadness, but from joy.”
Many of these boys and young men come from homes where there are few material possessions, sometimes even no plumbing. They live in houses, make-shift sheds, or cramped and hot urban rented rooms. Camp is so much more than a fun time for them. It’s a celebration of life, a communion of children and young adults who share a common pain, and a foundation for the future. It gives them hope that things will change. Blood, sweat and tears? Bring them on: the blood and sweat you cannot avoid at a hemophilia camp in the tropics. The tears are a delicate leaking of innermost feelings of gratitude– for being alive and for being loved.
This camp is one of the greatest things I have ever been involved with, and nothing makes me happier than to see the boys together, as friends, as mentors, sharing life and memories, and preparing to raise the next generation. I am here till Wednesday, when I leave on a 8 hour bus trip to Haiti–stay tuned!
I’ve been to a lot of places recently, and one of the most interesting ones was the GTC Biotherapeutics farm in Charlton, Massachusetts, on Friday, May 21, to see transgenic goats.
We wrote about transgenic animals in the February issue of PEN, when I discussed hemophilia products that are being developed now. Factor produced through transgenic animals may one day become a source of factor concentrate. And if production proceeds as hoped, transgenic animals may represent a high volume and thus low-cost way to produce factor and other proteins. What are transgenic animals? These are animals that have been genetically modified to express human therapeutic proteins in their milk. In other words, human factor can be collected by milking these animals. The source material is raw milk. And once the proteins are collected and purified, they can be used to treat diseases and genetic or metabolic disorders in humans.
Now, the goats located on the 167 acres that bridge the towns of Charlton and Spencer, Massachusetts, are not being raised to create factor, although factor IX is being produced by transgenic pigs in Virginia, and factor VII is being made by transgenic rabbits in France. The goats we visited express the protein used in ATryn®, a recombinant form of human antithrombin. Atryn® is the first transgenically produced therapeutic protein to receive FDA approval and the first recombinant antithrombin approved in the U.S. So as wild as this all sounds, GTC already has an FDA-approved, transgenically produced therapeutic in the marketplace. And GTC is hoping to initiate a clinical trial for their factor VIIa product later this year.
I requested a tour, and was enthusiastically greeted by Ashley Lawton, Vice President, Business Development. Before I entered the building, I had to dip my shoes into a disinfectant solution, to kill any microbes. Of course, I was wearing sandals!
Safety was stressed at every part of the two-hour tour.
Ashley told us that the goats originated from New Zealand, because this is one of the few countries free of scrapie, a fatal and degenerative disease in sheep and goats. Why use goats and not cows? Goats produce more milk and their milk has a high protein content; they also have a four-month gestation period. And they are relatively easy to breed and maintain.
GTC is a pioneer in the field of transgenic technology, and because it involves making human therapeutic proteins, regulatory agencies want extensive documentation. Everything done to the animals, from having their hoofs cleaned to operations, is documented fully. . Dr. Bill Gavin, General Manager of Operations and chief veterinarian, joined our tour and told me, “Because we were a new technology… we were held to an even higher level of safety.”
We toured the labs where the genes are spliced into the embryos. We traveled to the barns where the goats are penned. Somehow I expected sterile, see-through cubes with goats hooked up to machines. Instead, we saw adorable goats comfy in stalls, much like you’d see on any farm. The “kids” were cuddled together. Young adults were able to mingle and hang together; they even had toys to play with like bouncing balls. Goats love to climb, and these had cubes to scale.
Goats are fascinating. They are curious, sociable and always hungry! They’ll nibble on anything and eat just about anything. I couldn’t go too near them but got close enough to see these are probably the best cared for goats on earth.
I’ve been invited to view the pigs in Virginia that are being researched currently to produce factor IX; after this trip I think I need to go check it out. Actually seeing the goats and the technology made this seem more than just a pipedream. Perhaps the biggest revelation is that we would not “drink” the treatment, which I actually believed! Once the protein is purified from the milk, it will be freeze-dried and prepared as an injectible, biological product, very much like the factor concentrates available on the market today.
I know there are those in our community who might think this is unfeasible. But for me, this is a ray of hope. Transgenic animals might be particularly attractive as a way to treat hemophilia in developing countries, where there is great need for a low cost product, and plenty of it. Do you know which countries are the top five in population?
In order: China, India, US, Indonesia, Brazil. Four of the five most populated countries on earth are developing countries. So it stands to reason that a huge population of people with hemophilia are underserved and in need. This wonderful tour on a warm spring day left me hopeful that plentiful help for them might someday come from this fascinating new technology from humble farm animals.
Interesting Book I Just Read The Seven Powers of Questions By Dorothy Leeds This book asks questions, actually: why do we talk so much and not listen? How can we better focus and learn? What are effective ways to ask questions? Leeds covers a lot of ground about how we communicate, mistakes we make in trying to form relationships (whether business or personal), and how to be a better listener. Asking questions makes us better listeners, helps us to focus, diffuse defensiveness in others, calms situations. She notes the things that make us poor listeners: having preconceived ideas, jumping to conclusions, being emotionally charged. Questions help break down those barriers, and make us more open to listen, and then to think. This book got off to a very weak start (I think it was opening with a not-so-good quote from the 1960s Star Trek TV show [and I consider myself a fan]) with a plethora of cliché quotations from oft-referenced works (Ask a better question to get a better answer: how many times have I heard that?) and also had a weak ending, by evolving into a “Where is your entire life going and how will you get motivated to be an empowered person and make your dreams come true…” But overall there is material that is vital to know and this book will be welcome to read if you are new to self-help books or any book on communication. Two stars.
I’m very happy to report that the Inhibitor Summits are back this summer. Two Summits are scehduled, one in Houston and one here in Boston.
August 5-8, 2010 — Houston, TX August 19-22, 2010 — Boston, MA
Come join other people with hemophilia A or B with inhibitors and their families for a weekend of education designed to improve your overall health and quality of life.
REGISTER NOW! http://www.nhfinhibitorsummits.org/
From the NHF announcement: Having an inhibitor can seem overwhelming at times that even day-to-day life can be a challenge. This can affect your well-being in ways that only other people with this condition can understand. The annual Inhibitor Education Summits connect people with inhibitors, their caregivers and members of their support network with expert healthcare professionals. They also connect you with others who have been where you are–people who can share their experiences or suggest a coping skill.
New this year:
Multiple educational tracks Exciting Youth Camp activities planned for kids ages 4-12 Coping mechanisms for improving the psychological well-being of patients and their caregivers To register or for more information, visit the NHF Inhibitor Summits Web site, call 877-560-5833, or e-mail inhibitorsummits@hemophilia.org. Travel and lodging assistance is available for eligible patients and their caregiver(s).
Atención: los representantes hablan español.
This educational program series is provided by the National Hemophilia Foundation and supported by an educational grant from Novo Nordisk.
Hope to see you there! Register today!
Great Book I Just Read Tears in the Darkness Michael and Elizabeth Norman This book, about the horrific Bataan Death March in the Philippines in World War II surprised me. It’s told mostly through the eyes of ordinary soldiers, one in particular, Ben Steele, a 20-something year old, budding artist from Montana. The book chronicles the war-fever (Steele’s own mother encourages him to sign up for military service), the surrender of 76,000 Americans and Filipinos to the Japanese in the Bataan peninsula, and the infamous death march that led to the starvation, dehydration, beatings and executions of so many. Japanese military brutality is on display with a candidness that is chilling. The suffering Ben Steele endures, along with his fellow prisoners, is almost not to be believed. Ben eventually becomes a POW, and becasue he is sick, is put in sick bay, where he bides his time be sketching what he sees. His illustrations are in the book, though it’s not always clear what the pictures are of. This is a sad tale of Japanese brutality and total American military abandonment of its own soldiers in their hour of need. How anyone survived the march is beyond belief. Eventually of course, Douglas McArthur (“I shall return”) does return and the Americans capture the peninsula. Interestingly, the Japanese side is told thorugh the eyes of commander Homma, who acts unaware of the rtagedy that unfolded under his watch. It’s almost sad to see what happens to him and his family. A must read for WWII fans. Four stars.
Today was a field trip, outside of the bustling, clogged streets of Nairobi. We headed to Murang’a, a town about 90 minutes away, off on the highways pitted with deep and numerous potholes. The shoulders of the highways are crumbling and soft so in dodging the potholes, we have to be careful not to veer too close to the shoulders or we will need up in a ditch.
You may think Africa is hot (the very name means “Away from the cold”—A frika), but Kenya is quite pleasant, with cool breezes, mostly dry air, and even chilly in the evening. No wonder so any settlers came here and stayed. The climate, the rich red soil, the friendly people make Kenya a country where people dream of living.
Maureen Miruka, mother of two-year-old Ethan and founder of the Jose Memorial Hemophilia Society, was our fearless driver. With us also was Paul, the 24-year-old administrator of the Society. How nice that Maureen hired him—he has hemophilia and many of the young men with hemophilia cannot hold down jobs. Remember that there is no factor in Kenya unless it is donated, and the donations are only enough for a few.
Our first stop was the Murang’a District Hospital, where we met the gracious Senior Nursing Officer Danny Mengai. Joining us later was Dr. Nguyo. Maureen had met them previously, explained about hemophilia and this time brought with her their very first ever donation of factor! This is factor that my organization Project SHARE had donated to her organization. This was the kind of teamwork and outreach I like to see. Imagine: Murang’a has a higher than normal concentration of people with hemophilia and there has never till now been any factor in the hospital. And you can bet that fresh frozen plasma is hard to come by as donating blood is not a tradition in Kenya, or in any African country.
I learned today that a big teaching opportunity for the JMHS would come in December: this is when the vast majority of circumcisions are done. Why? I asked. For religious purposes? No, Maureen replied: school holidays. Boys are circumcised around age 12 and this is when we can get referrals for bleeding disorders to the Society. Dr. Nguyo assured us he would check with Maureen at that time, and also refer anyone suspected of a bleeding disorder.
Back in the Toyota and then on to visit patients. This was our very first official field visit—sorry, the second. We must give Paul credit. He had visited previously by himself to do the groundwork, and take down patient information for Save One Life. And he did an excellent job! Our goal is to start enrolling patients from Kenya, and ask anyone reading this blog to consider sponsoring a child form Kenya. The needs are terribly great and it won’t take much to change their lives.
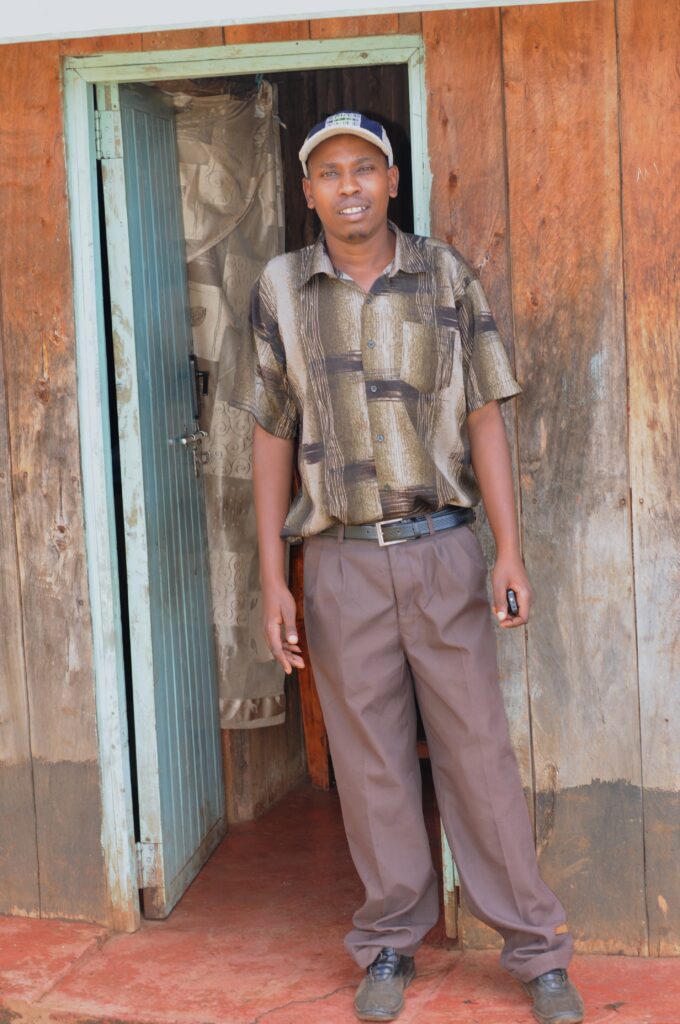
Take Peter for example. Just down the street from the hospital, on a red dirt road, in a small apartment lives Peter, age 19, with hemophilia. He is thin and speaks softly, like most Kenyan boys. He was so curious about his condition, and wants to be a doctor when he grows up, “So I can help other people like me. Because I know how they suffer.”
That’s an understatement. I am not sure we can understand how much these children suffer, with no relief, night after long and desperate night. (Photos: Peter; his kitchen; Me with family)
Let’s imagine what it is like for Peter when he has a bleed. There’s no money to get to the hospital. He has no crutches, of course, no wheelchair. He remains housebound. He tries to hide it from his distraught mother. She is single, and caring for Peter, and his brother, who has emotional problems as well as hemophilia, and also has adopted her two nieces, abandoned by her sister. The mother makes only about $20 US a month washing clothes and housekeeping for people. Peter’s bleed worsens, as does his pain. At night they all sleep in one room (the only other room they have, which also functions as a “kitchen,” because it has a charcoal pot in it) probably a few of them crammed into one bed. If anyone moves, this sends shooting, excruciating pain from the bleeding joint. Peter can’t get up and watch TV as a distraction, or Facebook, or do Wii, or pop a painkiller, or grab ice from the freezer or treat himself to a Coke. They don’t have a refrigerator, and own nothing but the basics—a table, chairs, couch, a bed or two, a boom box. If he gets up he’ll wake everyone. And in Africa, kids don’t whine and demand and complain. They suck it up with dignity. He lies there all night, trying to control the pain. The last thing he wants is for his mother to find out, which will add to her worry and suffering. He learns to be stoic and fight the pain, because there is simply no other choice. This bleed goes on day after day and night after night. It finally subsides… until next week, when this scenario happens all over again.
This is his life, and he cannot imagine any other.
We record his family history, ask him about his schooling, and his plans. We learn that his brother is in a mental ward. The entire family was terrorized last year during the post election violence. Thugs entered their home, set it ablaze, and chased them out into the streets. This is a nice, Christian, impoverished family, with two young men with hemophilia; they deserve nothing of what has happened to them. The younger brother, already fragile, is suffering from post-traumatic stress disorder. We make plans to go visit him. He’s ready to come home, but the family has incurred $350 in fees and like most developing country hospitals, the patient is not released until the bill is paid. You hear that right. Peter’s brother could be there indefinitely. We’ll see about that.
Who wouldn’t want to sponsor Peter? What a lovely young man; so sensitive and sweet, so gracious and kind. If he were placed in America, there would probably be nothing he couldn’t accomplish with his winning perspective.
The road calls, and we soon leave, after first handing out some presents to the family. On to the next patient: Peter’s uncle, also named Peter. He is older, with a family: wife and two children. He lives, well, basically, in a jungle. We park by the side of the road, surrounded by banana plants, overgrowth, trees and vines. Someone actually lives in that thicket of vegetation. We pull over under a big tree and a crowd of children gather, from the other side of the street. They giggle and whisper, “Mzungu!” and cover their mouths. What does that mean, I ask Maureen. Maureen smiles and says, “White.” Not many people like me make it out here, I guess.
I dissolve our differences by hauling out my stash of Tootsie Pops. Never, ever travel in developing countries without them. They withstand the heat and luggage manhandling, and are beloved by everyone. I hand out one to each bystander and immediately have fans!
We should have brought machetes because to get to Peter the uncle, we have to step over rocks and push back the big banana leaves. A short walk down the twisty sort-of trail and we arrive at their plot of land. Such poverty.
A split-log home, tin roof, muddy ground. The floor inside the house is missing; it’s just mud. There is no electricity. There are indicators of various levels of poverty and this is one key: do they have electricity? Believe it or not, you can do without plumbing. An outhouse will do and most people in the villages have them. But when you don’t have electricity…. You might as well be living in the 1800s. No, even earlier, in this case.
This family owns nothing, nothing. No vehicle, hardly any furniture. A homemade chicken coop housed a few chickens that had no food or water and the heat was growing. I felt for them, sadly. They cackled unrelentingly. A dog was penned in the back, also in a homemade kennel, with hardly any ventilation, whining to be released. The children padded around barefoot, the wife was a bit cautious, not too friendly. (Photos: the outhouse; Peter with family)
I gave the children the customary Tootsie Pops, which they eagerly accepted, and a superball and a toy kitten that shook when you pulled his tail. They were frightened by the toy at first. Then they thought it hysterical, and they made it shake over and over. I had rescued some toys from the CVS store which operates right beneath my office. Apparently, they ditch whatever they don’t sell every month: perfectly good toys, baby items and medical items. I retrieved toys for kids, baby strollers, thermometers, heat wraps, you name it. Yeah, I am a Dumpster Diver and proud of it. Everything is neatly wrapped in clear plastic bags and in perfect, new condition. And these kids had a ball with the toys.
After our interviews with Peter, we headed for the next house. Also perched in a jungle-terrain, on a hill, Charles’s home at least has electricity. And the animals look well cared for. We were greeted by the father, Sampson, an elegant elder man, his wife, who eyed us warily, and later told us this was the first time she ever met anyone else who had a child with hemophilia (! She must be about 60), Charles and his new wife, Hannah.
Charles approached us on a crutch, with obvious crippled joints. But what a nice young man: age 24, speaking fluent English (Kiswahili is the national language but most educated people—meaning grammar school and high school—can speak English as Kenya was once an English colony). Charles shared so much with us: his hopes to return to college and study electrical engineering, because he has a knack to fix anything, and he longs to contribute to his family. His parents are elderly. How much longer can they work and support him? It’s such a source of shame for an African man to be supported by his own parents. Hannah was sweet and gave me a little tour of their farm. The animals were all housed in self-made, split-log cages, but really well done and humane. A cow, goats, chickens and a dog. As clean as can be for living in jungle-like surroundings. They don’t have a refrigerator and Charles could really use one for ice for his joints. He lives so far from any hospital and they of course don’t own any kind of transportation! Not even a horse.
We were so impressed with the family. So good, high hopes, willing to work hard. Charles needed $350 to get his school fees paid for so he can return and get his degree. He just doesn’t have that kind of money. People like him, Peter and all the others we met live day to day. It’s truly survival. And when thugs burn your house down, or the rains come and wash away your farm or crops, you are really threatened with starvation and just pure survival.
We just cannot imagine their daily lives. I have a hard time, and I have seen it in front of me. How do they do it?
And yet I never hear a complaint, or curse. The only think I hear are blessings: May God bless us for our work, may we have a safe journey, thank you for helping us. Now maybe you can see why I return over and over. Despite their poverty, they have a richness many of us in developed societies lack.
We parted on such happy terms, and we all chattered on the way back about what a diamond in the rough Charles was! Peter too, in a different way.
We visited two more families, Stanley, a grown man, and Derrick, a one year old and actually Paul’s nephew. By then it was really growing late and I was out of Tootsie Pops and just about anything else in my purse that I had given away.
Our last stop of the day was at a home of a better off family. They have a proper concrete home, electricity, and the father is employed as a teacher. The son with hemophilia neatly dressed with shoes. We had a nice courtesy visit, and afterwards, to show their appreciation, the mother presented Maureen with a magnificent rooster!
They popped the rooster into a plastic bag, tied the top and carried it out to the car, its crested head popping out. When they opened the “boot” (trunk), the animal lover in me sprung out. We just can’t put a rooster all trussed up in a plastic bag into a hot trunk! It was 90 degrees and we had a two-hour journey back on horribly bumpy roads! The poor thing…
So I rode with the rooster in my lap, all the way back to Nairobi for two hours at night, petting it as if it were a cat. The doorman at the Holiday Inn was pretty surprised when he opened my door to let me out!
I’d call it a successful day all around for Save One Life and Save One Rooster.
(Please consider sponsoring one of the families mentioned above! Just $20 a month. See http://www.SaveOneLife.net)
Today we met a very special person with hemophilia, who touched us deeply, and reminded us of why we do the crazy things we so—like driving about three hours outside of Nairobi, deep into the Kenyan countryside just to meet one patient. Well, this is why we call our nonprofit “Save One Life.” It’s all about one person at a time.
You cannot separate Simon’s story from the logistics. Sure, he has hemophilia, as does his brother. He’s 26. His wife left him, and he now lives on his mother’s farm. He has the usual untreated bleeds, and hobbles about on crippled legs. We wanted to meet him because we knew he lived in difficult circumstances. Total rural living; you might say primitive, if you judged him by the average American standards.
We headed out at 8 am with Maureen Miruka, founder of the Jose Memorial Hemophilia Society, driving. With us were Paul, a 21-year-old with hemophilia, impeccably dressed as always, and Jeff, our videographer. They picked me up at the Holiday Inn, and off we went.
Over two hours of driving on a highway, dodging the worst potholes you can imagine. The shoulders of the road drop swiftly, so we have to be careful not to veer off. It was like a high-speed obstacle course! Left, right, fast, slow, then the random speed bump. The speed bumps (or “sleeping policemen”) are not marked, and so blend in with the road, and can cause severe damage. The ride seemed to take a lot longer than two hours.
We took a short break to see the breathtaking Rift Valley, 3,600 miles long, and an important source of fossils.
We arrived in Nyahururu, far north of Nairobi, a bustling town. As always, the Kenyans are dressed well, and walking, walking, walking. It seems that everyone walks in this country. I was surprised to see a long line of young men with motorcycles, just waiting. This was local transport, and in a minute I would find out why.
We spotted Simon under a gas station sign, waiting for us. I gave up my front seat when I saw how painfully and slowly he was walking, to give him more room and excluded room. Simon would show us how to get to his home.
We turned the corner to Simon’s street. The street is a dirt road off the main road. The red, rich soil of Kenya covers every inch of this long road. Up we went, as the road ascended and we dodged not potholes, but regular bikes with massive loads of grass or wood, their drives pushing them resolutely upwards. Or women and children carrying huge loads of potatoes in sacks, supported by bands around their heads. Or cows, stumbling down the road into town.
We spun in the soil, which was muddy at times, and began to wonder how on earth Simon could manage this. We finally arrived at his farm, perched high on a hilltop with a spectacular view of Kenya. To get to his farm you must climb up another dirt pathway strewn with rocks.
The logistics of getting him help for a bleed are mindboggling. When Simon gets a bleed, this is what happens:
Simon, in pain, has to either walk down the dirt path to the dirt road, then walk over three miles on this dirt road, down the hill and into town. Then he has to wait for the local bus to drive him to Nairobi, to the only hospitals that know how to care for people with hemophilia. Our drive took over two hours, and that was going fast. On a bus, you can expect to take two to three times longer as it makes stops, and goes slower.
All the time, Simon is in great pain.
We arrived probably with our mouths gaping: the farm is rustic but pretty and what a view! His mother greeted us, but wasn’t smiling, the way Kenyans usually are when they smile. Indeed, the entire family was grim, and tight-lipped. “They are stressed,” Maureen said to me aside.
We sat inside the small home (we would call this a shed) where his mother lives. I glanced around and noticed the corrugated tin roof (nothing new there; this is a given in the developing world) and cardboard. The walls were split logs, and the “wallpaper,” or covering, was cardboard, through which the light peeped in.
We chatted with Simon a long while, recording his family history and discussing his bleeding pattern. This would give us the necessary information to register him with Save One Life and find him a sponsor. Jeff also gave him an interview, and Simon spoke in Kiswahili, the national language, as his English is very limited. He shared his frustration, not at hemophilia, but of the incredibly long distances he must cover just to get some kind of help.
It was clear to us all that Simon needed to keep factor at home. To my delight I learned that he had been taught to self-infuse. But the government of Kenya buys no factor, and so there rarely is any available. Imagine traveling all that way in terrible pain only to arrive at the hospital and be told there is no factor! Or, come back tomorrow for your FFP.
Simon’s mother surprised us with a wonderful home cooked meal: mokimo, a national dish. It was the only meal we would eat all day (and only my second meal in two days!!). Things started to lighten up a bit. We presented Simon with a gift of factor VIII; we shared how Save One Life would provide funds for transportation. And we pledged somehow we’d keep him stocked with factor. By the time we shuffled back to the car, everyone was beaming, like a little ray of light brightening his future.
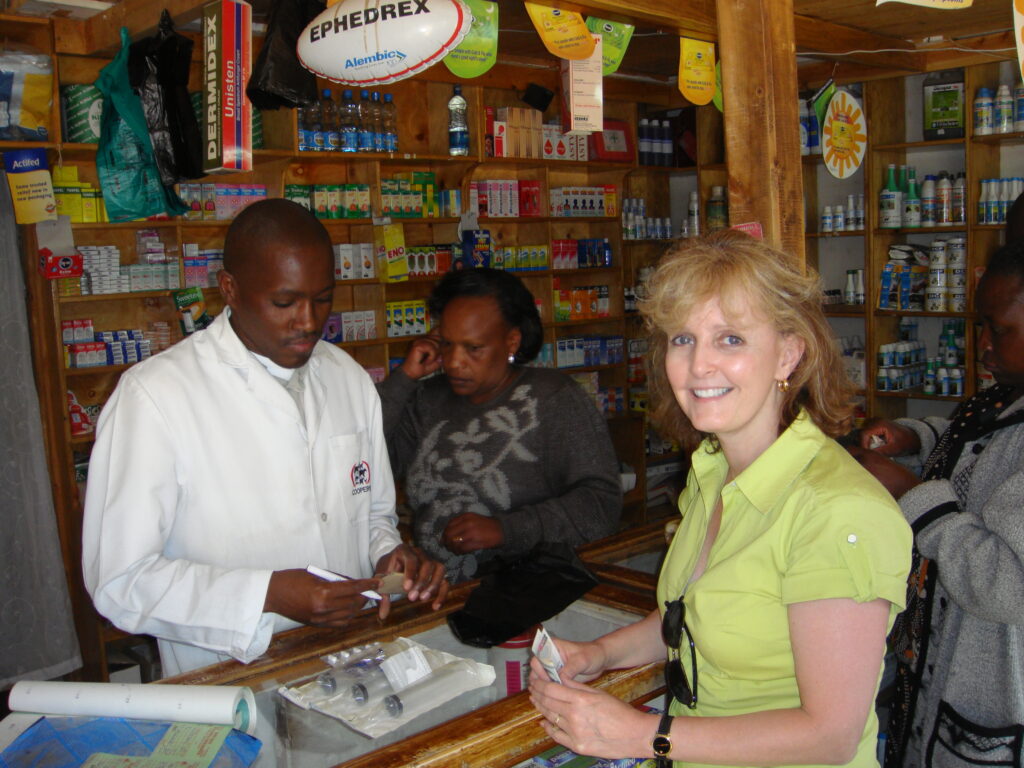
Before we left, we stopped at the local pharmacy where I bought Simon syringes, needles and medical tape. Things we so take for granted are not free here! And some cash so Simon could ride one of those taxi-motorbikes back up the hill to his home.
The ride back was both sobering and exciting. We had defined ways to help this very special man.
Our day was far from done. The ride back—three hours again—was only to plan what to do about another young man, age 21, hemophilia A, in a mental institution. He was placed there following the post-election violence that engulfed Nairobi last fall. This young man’s home was invaded, ransacked and then burned to the ground by electrified hoodlums, as many homes burned all around. I don’t know his whole story: perhaps he was chased, terrorized. Whatever it was, it left him so traumatized and depressed, he had to be committed. We heard he was able to leave now, following two months of treatment.
The problem? His mother, single, with two boys with hemophilia and two nieces, has to pay $340, a fortune, perhaps more than what she makes in a year. The son would not be released unless this was paid. This is the way it is in developing countries. We actually drove at twilight to go see him. We were allowed into the padlocked Men’s Ward, and the rank smell of human beings unable to care for themselves assaulted us. Lying on cot after cot were young men, about 25, all heavily sedated for the evening. The boy’s mother was with us as we tried to wake he son. He awoke and stared at us blankly, through drugged eyes. He looked so small and helpless on the old, thin cot. My God, I thought. This could have been my 22-year-old.
I made the only decision I possibly could; I gave the money to Paul, and tomorrow (Thursday) he would go with the mother and bring this poor child home, where his family could care for him.
This was a day of pure experience and exploration in the lives of two young men in desperate need. We cannot fix everything or everyone, but our motto at Save One Life is “To save one life is to save the world,” and that works just fine for me.
Simon
Maureen, founder of the JMHS
Laurie buying ancillaries for Simon
HemaBlog Archives
Categories
Download Now
Would you like to be added to our email list to continue to recieve future editions of PEN in PDF format?
LA Kelley Communications - You are leaving our site
You have clicked on one of our advertiser’s links. Our provision of a link to
any other website or location is for your convenience and does not signify
our endorsement of such other website or location or its contents.