Puerto Rico: Mi Corazón se Rompe

My heart breaks. I sit at home tonight, trying to imagine what it would be like to have my house half submerged in water, a fallen tree slicing through one bedroom, my clothing and photographs ruined, the sewers backing up into the rushing water from the overflowing streets, my two cats missing and presumed drowned, my daughter huddling with me, unable to contact anyone for help because all electricity is out, and our cell phones were lost during the roaring winds, downed lines, and river of rain left in the wake of a massive hurricane. Our beds are soaked; food in the fridge ruined and submerged in the muddy water; medicine soaked; streets impassable.
No way to contact relatives; no way to call for help. Creatur es of the night and underground now emerge to gasp for air: snakes, spiders, rodents, carrying disease and threat of bites.
es of the night and underground now emerge to gasp for air: snakes, spiders, rodents, carrying disease and threat of bites.
 es of the night and underground now emerge to gasp for air: snakes, spiders, rodents, carrying disease and threat of bites.
es of the night and underground now emerge to gasp for air: snakes, spiders, rodents, carrying disease and threat of bites.Society has broken down and we wait and wait in the dark, throughout the day, and into the next night, for help of any kind. We’re hungry and thirsty, dirty and shivering. And alone.
This is the situation for so many families in Puerto Rico, where not just one town, or even just the capital was pummeled by Hurricane Maria, but the entire island. This tropical semi-state, a possession of the US, a warm, colorful albeit poor place, dependent on tourism and the welfare of the mainland, is now a ravaged
wasteland, and it will take months, perhaps years to rebuild.
wasteland, and it will take months, perhaps years to rebuild.
 I feel for Puerto Rico so much, probably even more than for the states of Texas and Florida. The needs in PR are massive; they were in economic trouble long before Maria hit; it was so bad that many Puerto Ricans were leaving the mainland in droves, for better medical care and education. And PR is an island, making rescue and ferrying aid so much more challenging.
I feel for Puerto Rico so much, probably even more than for the states of Texas and Florida. The needs in PR are massive; they were in economic trouble long before Maria hit; it was so bad that many Puerto Ricans were leaving the mainland in droves, for better medical care and education. And PR is an island, making rescue and ferrying aid so much more challenging.I have been going to Puerto Rico since 1998, when I first visited to check out the hemophilia situation there. (Read our in-depth article about hemophilia in PR here) Though they belonged to the US, and were entitled to US funding for healthcare, they only used one factor product, a plasma-derived! Through the years, helping the newly resurrected Puerto Rico Hemophilia Association, we all helped bring patients together and pressured the medical community to investigate new products. The result? A variety of products in the mid-2000s, including recombinant, and a strong, patient-driven hemophilia association. I watched this group form, develop and grow into a powerhouse.
Mother Nature has set us back, but has not defeated us. I say “us” because I am still with PR. At the NHF meeting in Chicago just in August, I met with one of the island’s pharmaceutical reps and we talked about hosting another visit, to do more leadership training, to keep things moving forward. It will have to wait.
For now, we urgently need to get supplies into PR. Because our company and especially Zoraida, director of Project SHARE and who is from Puerto Rico originally, deals with humanitarian shipments, we will be contacting the manufacturers to see who is donating factor to the hospitals. We will be asking our readers and friends on Facebook to consider donating material supplies and necessities.
But… many people hesitate to donate to a place like Puerto Rico. Will the donations go into the right hands? I get it. At Project SHARE we diligently follow each vial of factor to its destination. But what about clothing and supplies to Puerto Rico?
We have a way. Allison Plaud, a mother of a child with hemophilia I met on one visit (and who has since emigrated to mainland US), has assured me that one of her trusted friends, a businessman, is collecting donated items and will be shipping them on Saturday to PR.
We endorse Allison and her friend, and beg everyone in the hemophilia community to donate items to ship.
Here are the items, and

where to donate!
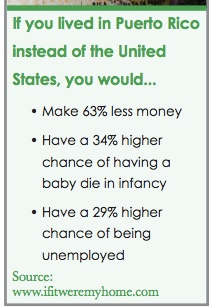
And here is the situation in Puerto Rico.
I am haunted by the images, and by their suffering. Forget athletes kneeling, politicians sniping. Let’s be real Americans and do
what Americans are best known for: being the first to help. Puerto Ricans are Americans and we must help them. This
is when I am proudest to be an American!
what Americans are best known for: being the first to help. Puerto Ricans are Americans and we must help them. This
is when I am proudest to be an American!







