If your dreams do not scare you, they are not big enough. —Liberian President Ellen Johnson Sirleaf
I’ve never met anyone in my life–and I have met some pretty amazing people in my several careers–who dreamed a dream, set the course, followed through against all odds, and made it happen in the way that Chris Bombardier has. If you met him, and I hope you do, you would be thunderstruck that this shy, extremely humble young man will soon conquer the Seven Summits.
Chris Bombardier
And not just achieving an incredible goal that only about 450 people in the history of the world have ever done. No one has ever done this who has a bleeding disorder. No one might ever repeat this in my lifetime. We are witnessing history in the making! In hemophilia terms, this ranks right up there with landing a man on the moon.
Chris leaves tomorrow, Christmas Day, for the last adventure on this journey that has consumed the last few years of his young life. I interviewed him last week, before the holidays. How did he feel?
“I’m looking forward to my last summit bid—Mt. Vinson. I’m leaving my wife and family on Christmas Day to basically a frozen desert. On December 29, I’ll leave from Chile to fly to the Antarctica continent. I’ll land on Union Glacier, and from there we will get a flight to the mountain base camp, but everything depends on the weather. Base camp is a few miles from the base of Vinson. We’ll stay at camp, sort out our gear, then start the hike.”
I actually traveled with Chris last March when we trekked to Everest base camp, which took 9 days. It was freezing by the time we got to base camp. I stayed three days but Chris had to stay about a month to acclimate, as Everest is 29,000 feet. How long will it take to summit Vinson, which is 16,050 feet?
“It should take us about seven days total. Our challenges this time isn’t the lack of oxygen, like on Everest, but the weather and temperatures. Temperatures can be all over the place, but pretty much it will be below zero all of the time. The wind is the worst here. The wind brings the temperature down, and you can easily get frostbitten.”
With Chris will be his trustworthy guide Ryan Waters, founder and president of Mountain Professionals of Colorado. Ryan’s guided Chris on 5 of the Seven Summits. This one will make it 6! This trip, like the Everest one, is being fully sponsored by Octapharma, which manufactures blood-clotting products like Nuwiq® and wilate®.
What’s even more impressive is that Chris has undertaken these climbs not to make history or for personal glory. He knows that it will gather world-wide attention, but not for himself, but to highlight the inequity in treatment for those with hemophilia in developing countries. He worked in Kenya, before he started his climbs, helping to establish a lab in Eldoret, and what he saw convinced him he had to draw attention to how much people with bleeding disorders suffer. Chris and I met in 2011 at a NACCHO conference; after I gave my talk about our work in developing countries helping people with bleeding disorders, Chris told me he wanted to do the Seven Summits–just a wild dream he had to help bring attention to this problem. A lover of mountains myself, and avid reader of those who undergo extreme hardship while exploring (David Livingston, I presume?) and achieving (Mallory, because he’s there), and reading everything I could get my hands on related to summiting anything, I told Chris go for it, and I will help in every way humanly possible. He did all the training and work, and I’ve been cheering him on! And Chris joined our board of directors at Save One Life.
Chris wants to dedicate this climb to raising money for our scholarship program. He writes,
“With your support, I know I can make this climb successful!
“No longer can anyone say that someone with hemophilia can’t climb Everest, Vinson or reach any dream, as long as they have with proper treatment, training and medical care. By standing on these Seven Summits, I hope to show what is possible. I hope by holding the Save One Life banner on each summit we can show the world that only 25% of people living with hemophilia even have access to adequate treatment to chase dreams. Let’s help everyone aim for their dreams by helping to raise $16,050—the height of Vinson— for our scholarships!”
Chris is doing the hard part; let’s help him achieve this last mountain and goal by raising $16,050! If he can climb Vinson, then we can raise the money!
Inhibitors can be a devastating response to infused factor. It’s good to review what they are, how they form, and what treatment is available, even if you or your loved one do not have an inhibitor. Below is information on what we know about inhibitors.
Read and learn!
Laurie
This is a paid public announcement from Shire and does not constitute an endorsement of products or services. When you click on the links in this blog entry, you will be directed to the Shire website. LA Kelley Communications always advises you to be a savvy consumer when contacting any company; do not reveal identifying information against your will.
The development of inhibitors adds great challenges to managing hemophilia
As you may know, factor proteins are a vital component in the blood-clotting process and help to stop or control bleeds. However, if you are missing one or more of these factors, your body is unable to effectively manage a bleed.1-3 Factor treatment temporarily replaces the missing proteins in your blood, working within the natural blood-clotting process to help create the necessary clot and stop a bleed.1-6
Treatment of inhibitors is one of the greatest challenges in hemophilia today.7 Some patients develop antibodies called inhibitors that actually stop, or block, factor VIII (FVIII) or factor IX (FIX) function in the blood-clotting process.8,9 In fact, up to 33% of people with severe hemophilia A develop an inhibitor to treatment, while 5% to 10% of patients with mild to moderate hemophilia A develop an inhibitor.9-11Inhibitors are less common among people with hemophilia B, affecting only 1% to 6% of individuals. Bleeding is more difficult to manage in patients with inhibitors because they do not respond to standard factor replacement treatment. Inhibitors attach to the replacement factors, making the treatment ineffective.11
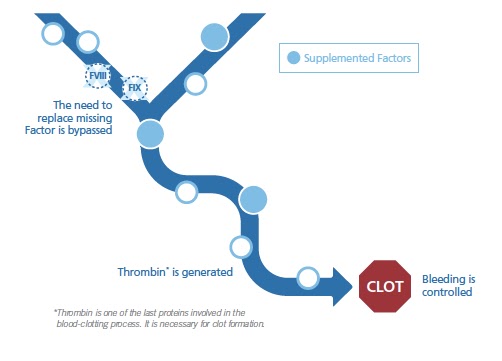
To avoid the need to replace missing factors, patients with inhibitors need a different treatment approach, such as the use of bypassing agents. Bypassing agents are made up of factor, or a combination of factors that are naturally found in the body’s blood-clotting process. Bypassing agents offer an alternative treatment approach because they go around, or bypass, the need for FVIII or FIX while supplementing factors involved in the blood-clotting process.8,11-14
This chart is a simplified visualization of Bypassing Agent activity in the blood clotting process.
One way to think about the role of bypassing agents in the blood-clotting process is to compare it to a light switch:
Activation
Turning the light switch on—Before a bleed occurs, the process remains off but available when needed. When a bleed begins, the process is turned on. After infusion, bypassing agents are available to help control/manage the bleed.
Inactivation
Turning the light switch off—Once the bleed is managed, the blood-clotting process is inactivated.
The unused bypassing agent factors are eliminated from your blood. This inactivation step is very important. Unchecked thrombin generation could lead to risk of blood clots over time.
By working within the body’s natural mechanisms, bypassing agents are able to help stop a bleed in 3 tailored ways: when the bleed occurs, where (the site of the bleed), and how—by helping to form a more stable clot to help control the bleed.12,15
Bypassing agents provide options for individualized treatment.1 Currently, there are 2 bypassing agents available to treat people with inhibitors, and response to either treatment option may vary.15,16 In a study published in the peer-reviewed journal Blood, it was shown that 60% to 67% of people responded in the same way to each bypassing agent. These patients either responded to both bypassing agents or did not respond to either bypassing agent. However, up to 40% of people responded to only one bypassing agent and not the other in the first 12 hours after an infusion. The difference in patient response reduced from 7.3% after 48 hours.17
There are serious risks of blood clots with the use of bypassing agents.15 You should be monitored for the development of blood clots. If you experience any side effects while using a bypassing agent, call your healthcare provider right away.
Bypassing agents are infused intravenously, making the proteins needed for clotting immediately available for use.1,12,18,19 Bypassing agents may be used in the following scenarios:
PROPHYLAXIS
Infuse routinely to prevent bleeds1
ON DEMAND
Infuse when needed or to control breakthrough bleeds1
SURGERY
Infuse to prevent/manage bleeds during or after surgery 8, 20
It is important to work with a healthcare provider to develop an individualized treatment plan. A healthcare provider can tailor the dose and frequency of bypassing agents to fit with your lifestyle, depending on the severity of a bleed or the type of surgery. For example, if you have a mild bleed, or a minor surgery, your healthcare provider may adjust your dosage and/or frequency of bypassing agents accordingly. If the bleed is more severe, or you are having a major surgery, then your dosage and/or frequency would be increased accordingly.8,15,20
Bypassing agents are backed by a long history of use. Healthcare providers and patients have consistently relied on bypassing agents for over 40 years.21,22 With substantial bleed reduction benefits and extensive clinical experience, bypassing agents are considered a well-studied and established treatment option for hemophilia patients with inhibitors.15,21-23
Shire has been dedicated to pursuing advancements in hemophilia for more than 60 years.24 As a leader and innovator in hemophilia research, we offer a vast array of patient programs and support—all of which are proudly brought to you by our dedicated people.
EXPLORE THE POSSIBILITIES: To learn more about the treatment of patients with hemophilia A with inhibitors using bypassing agents, talk to your healthcare provider.
Peyvandi F, Garagiola I, Young G. The past and future of haemophilia: diagnosis, treatments, and its complications. Lancet. 2016;388:187‐197.
2.
Antovic A, Mikovic D, Elezovic I, Zabczyk M, Hutenby K, Antovic JP. Improvement of fibrin clot structure after factor VIII injection in haemophilia A patients treated on demand. Thromb Haemost. 2013;111(4):656‐661.
3.
Hvas AM, Sørensen HT, Norengaard L, Christiansen K, Ingerslev J, Sørensen B. Tranexamic acid combined with recombinant factor VIII increases clot resistance to accelerated fibrinolysis in severe hemophilia A. 2007;5:2408‐2414.
4.
Johari V, Loke C. Brief overview of the coagulation cascade. Dis Mon. 2012;58:421‐423.
5.
Lenting PJ, van Mourik JA, Mertens K. The life cycle of coagulation factor VIII in view of its structure and function. Blood. 1998;92(11):3983‐3996.
6.
Factor Replacement Therapy. Canadian Hemophilia Society. http://www.hemophilia.ca/en/bleeding-disorders/hemophilia-a-and-b/the-treatment-of-hemophilia/factor-replacement-therapy/. Accessed December 1, 2017.
7.
World Federation of Hemophilia. What are inhibitors? https://www.wfh.org/en/sslpage.aspx?pid=651. Accessed November 9, 2017.
8.
Leissinger CA. Prevention of bleeds in hemophilia patients with inhibitors: emerging data and clinical direction. Am J Hematol. 2004;77(2):187‐193.
9.
World Federation of Hemophilia. Guidelines for the management of hemophilia, 2nd ed. World Federation of Hemophilia, Montreal, Quebec, 2012.
10.
DiMichele DM. Inhibitor treatment in haemophilias A and B: inhibitor diagnosis. Haemophilia. 2006;12(suppl 6):37-42.
11.
DiMichele DM. World Federation of Hemophilia website. Inhibitors in hemophilia: a primer. http://www1.wfh.org/publication/files/pdf‐1122.pdf. Published 2008. Accessed November 9, 2017.
12.
Ananyeva NM, Lee TK, Jain N, Shima M, Saenko EL. Inhibitors in hemophilia A: advances in elucidation of inhibitory mechanisms and in inhibitor management with bypassing agents. Semin Thromb Hemost. 2009;35(8):735‐751.
13.
Retzios AD. The new and improved (?) activated factor VII molecules. Bay Clinical R&D Services. 2001:1-41.
14.
Berg JM, Tymoczko JL, Stryer L. Many enzymes are activated by specific proteolytic cleavage. In: Biochemistry. 5th ed. New York, NY: WH Freeman; 2002. https://www.ncbi.nlm.nih.gov/books/NBK22589/. Accessed November 9, 2017.
15.
Shapiro AD, Hedner U. Advances in bypassing agent therapy for hemophilia patients with inhibitors to close care gaps and improve outcomes. Ther Adv Drug Saf. 2011;2(5):213‐225.
16.
Hoffman M, Dargaud Y. Mechanisms and monitoring of bypassing agent therapy. J Thromb Haemost. 2012;10:1478‐1485.
17.
Astermark J, Donfield SM, DiMichele DM, et al. A randomized comparison of bypassing agents in hemophilia complicated by an inhibitor: the FENOC Study. Blood. 2007;109(2):546‐551.
18.
Hemophilia Federation of America. Treatment of hemophilia. http://www.hemophiliafed.org/bleeding‐disorders/hemophilia/treatment/. Accessed November 9, 2017.
19.
Hedner U. Recombinant activated factor VII: 30 years of research and innovation. Blood Rev. 2015;29(suppl 1):S4‐S8.
20.
Santagostino E, Escobar M, Ozelo M, et al. Recombinant activated factor VII in the treatment of bleeds and for the prevention of surgery related bleeding in congenital haemophilia with inhibitors. Blood Rev. 2015;29(suppl 1):S9‐S18.
21.
Mehta R, Parameswaran R, Shapiro AD. An overview of the history, clinical practice concerns, comparative studies and strategies to optimize therapy of bypassing agents. Haemophilia. 2006;12(suppl 6):54‐61.
22.
National Hemophilia Foundation. Medical and Scientific Advisory Council (MASAC) recommendation regarding the use of bypassing agents in patients with hemophilia A or B and inhibitors. MASAC document #167. 2006.
23.
NIH Clinical Trials Registry. Ongoing and complete clinical trials using bypassing agents in hemophilia patients with inhibitors. https://clinicaltrials.gov/ct2/results/detailsterm=hemophilia+a+with+inhibitors%2C
+hemophilia+b+with+inhibitors&recr=Closed&cond=hemophilia+a+with+inhibitors%2C+hemophilia+b+with+inhibitors. Accessed November 9, 2017.
24.
Higgins MC. Career imprints: creating leaders across an industry. 2005.
At LA Kelley Communications, we are devoted to providing helpful tools and resources to families with hemophilia. We have highlighted below two exciting Pfizer Hemophilia resources for you or your loved ones. The first is an innovative video game that gives children the opportunity to learn about their hemophilia by participating in a stimulating gaming experience. The second is the first wearable made for patients with hemophilia that offers an easy-to-use, comprehensive tool to track activity. The wearable integrates with Pfizer’s existing HemMobile® app, allowing users to log bleeds and infusions, monitor their factor supply, and set appointment reminders. Please read below to see if these exciting resources are right for you or your family members.
Enjoy!
Laurie
This is a paid public announcement for Pfizer and does not constitute an endorsement of products or services. When you click on the links in this blog entry, you will be directed to the Pfizer website. LA Kelley Communications always advises you to be a savvy consumer when contacting any company; do not reveal identifying information against your will.
HEMOCRAFT™, a virtual world designed for the hemophilia community
HEMOCRAFT is a video game developed to educate and inform younger patients with hemophilia about the importance of staying prepared and sticking to their treatment plan.
HEMOCRAFT modifies the popular Minecraft™ game to send players on adventures in a world where they have hemophilia
In the game, players interact with a treatment team to learn about the importance of staying prepared for activities
As part of their quest, players must find components to create infusion kits that help their factor levels stay elevated throughout their adventures
HEMOCRAFT was developed through a partnership between Pfizer Hemophilia, Drexel University, the National Hemophilia Foundation, and members of the hemophilia community
HEMOCRAFT is a trademark of Pfizer Inc. Minecraft is a trademark of Mojang Synergies AB.
HEMOCRAFT is provided for educational purposes only and is not intended to replace discussions with a health care provider, nor is it intended for curing, treating, seeking treatment for, managing, or diagnosing a specific disease, disorder, or any specific health condition.
Intended for US audiences only.
The HemMobile® Striiv® Wearable—the little app that could, with a wearable that can do even MORE
The custom Striiv® Wearable, when paired with HemMobile, offers activity tracking features to help patients with their hemophilia.
Wearable device monitors patient’s daily activity, heart rate, and number of steps to track intensity of activity
Allows patient and treatment team to have better discussions about intense activities, staying prepared, and managing hemophilia
HemMobile is not intended for curing, treating, seeking treatment for, managing, or diagnosing a specific disease, disorder, or any specific health condition. Pfizer will not have access to any personal information you enter into HemMobile.
After ten long years, I am returning to the second developing country I ever visited for hemophilia, and one I feel very close to–Pakistan. Just as I landed in Dubai, after a 12 hours flight, there were reports of protest throughout the country. It was serious: Facebook was even shut down for the first time in its history there. My Pakistani partners wondered if I should continue, as the airport road in Karachi had been closed, but after a flurry of emails, we all agreed I should continue.
I was pulled out of a long customs line by Asghar Ali, who works at the airport and has a son Rana, with hemophilia. As he put me on the fast track, I was through in no time. My friends hematologist Dr. Tahir Shamsi and Mr. Alam Zaidi, who has a son with hemophilia, were there to greet me in the cool early morning air—it was 6 am. I was staying with the Shamsi family, and it was so nice to be back in their home, after 10 long years.
After a rest, we all headed to the beach with the whole family–kids, wives and one grandchild!. It was fun! I’ve been here twice before on previous trips, once including the Shamsi family in 2007. It was hot and sultry. Camels waited for riders, decorated with colorful reins and enormous saddles with frames; horses, which I never saw before, stamped impatiently in the sand.
I mounted a white horse, which was compact and wiry. The owners walked them up the beach, then asked in sign language if I wanted to ride it by myself. I wasn’t really sure; was the saddle tight enough? The stirrups the right height? I finally said ok, and the man just said “Urdu,” motioning to the horse. What—the horse only understood their language Urdu? Then he slapped it on the flank and off we went! It was glorious! Galloping on this small horse on a beach at the Arabian Sea!
Next—camel ride! I loved how it stands knees first. That was a relaxing ride, though it lurches and then sometimes trots to catch up to the guide. I was a bit sunburned but what a great way to enter back in Pakistani culture and this nice family.
Monday November 27, 2017
Pakistan is the sixth most populous country in the world, but ranks 149th among 188 counties according to the UN, in sustainable healthcare-related goals. Keep that in mind as you read how a dedicated group of patients and their healthcare providers are trying to save their people with bleeding disorders and revolutionize care in this fascinating and ancient country.
Today I visited the Husaini Blood Bank, one of the very first stops when I first visited this country in 1999. Then, everything was so exotic and different, so strange. Pakistan was rather insulated from the world, prior to the US Iraq invasion of 2003. In 2007 I saw much US military presence. On this trip, none at all.
Alam Zaidi picked me up at Tahir’s house; as he got out of the car, the back two doors opened and out stepped two beautiful young people: daughter Fatmid, and son Abbas, both of whom I had met when they were children. Abbas, a teacher, is a handsome young man with hemophilia, dressed in a tailored suit, tall. Fatmid is lovely—a journalist.
The blood bank was not far, but what a far cry from my first visit! This was a new building, sparkling clean, modern and welcoming. Everything gleamed: chrome, glass and marble. The spry Dr. Jafry is ageless, and is still there as head of the Karachi branch. I met his team and we took a tour through the center. Blood banking is my weakest area, but I can appreciate the new equipment and that they now have hepatitis testing that reduces the waiting period from 70 days to 7 days! This means less chance of spreading the virus.The very first patients I met were two young men with hemophilia, receiving donated Eloctate from Bioverativ.
Magic! Laurie Kelley with kids
At last we met with the Save One Life children: 24 out of the 25 Save One Life beneficiaries we have registered there! A magician was performing so I sat on the sidelines and watched his slight-of-hand. He pulled a red ball out of thin air, made a wallet catch on fire, did rope tricks. The kids, big and small, loved it! Soon we started the ceremonies, as a small boy recited opening prayers from the Koran. The Karachi chapter did the introductions, and everyone made speeches. It was so kind that they showed photos from my 1999 and 2007 visit.
I met Mubashir, the factor 1 deficient boy I met in 2007, as two-year-old, and now 13! He speaks English and is so polite. I had factor FXIII medicine for them after the program.
The program was nice, covering the achievements of the Hemophilia Welfare Society Karachi, what Save One Life has done to help. Lots of photos ensued and then the kids were all given pizzas for lunch, while we met with the team and had our own lunch.
After this Alam and I drove to the Hemophilia Welfare Society Karachi,
Laurie Kelley, Dr. Jafry, Zahid Hussain and others
the NMO chapter. It’s small, but holds one fridge that contained some cryo, and the Biovertiv donation (see our article in PEN August 2017). Unfortunately, with the Biovertaiv donation, and the increase in infusions, have come inhibitors. Most are transient, thankfully. There are an estimate 4,000 with bleeding disorders in the Sindh province with only 460 identified and registered at this chapter.
Several of the staff were present. Raheel Khan is a phlebotomist with hemophilia, and works at Husaini. They actually have four paid staff, unusual for most hemophilia nonprofits in developing countries. Jawwad Shadid enters the data and gave me a demo; he has hemophilia. They have meticulous bookkeeping, and an excellent patient registry. I was most impressed! I saw this chapter back in 1999, and they have really progressed far, thanks from help from the WFH and Novo Nordisk Haemophilia Foundation. The donations from Bioverativ required all chapters here to up their game, get more organized and transparent and have standards of factor storage and distribution. Finally, we headed back to the Shamsi residence for the evening.
Laurie Kelley with Karachi Women’s Group
Tuesday November 28, 2017
Today Alam picked me up at 9:30 am, and we went to the Indus Hospital, and later, the institute that Dr. Tahir Shamsi founded, the National Institute for Blood Diseases (NIBD).
The Indus Hospital is breathtaking in size and scope. As we pulled into the grounds, a huge number of people waited in the chilly morning air. It was founded only 10 years ago, as a 150 bed hospital, dedicated to providing free care to anyone, regardless of class or gender. It’s growth has been explosive. It is now serving millions of patients for every type of medical problem. There are now eight hospitals in 5 cities. Care is absolutely free, so much so that this is a cashless hospital. True— no money ever exchanges
hands. Indus Hospital shows what is truly possible when one dreams big enough and has faith. This is also Pakistan’s first paperless hospital! Imagine! I was so stunned and impressed, I began thinking what I can do at my level to improve my services.
I met with the CEO Dr. Abdul Bari Khan, a gentle giant of a man, who despite his enormous achievements, is very humble and deflects praise. With us were some of his team, Dr. Izza and Dr. Chinoy (who was a classmate of my host, Dr. Shamsi). “You know Dr. Shamsi?” Dr. Chinoy asked me, amazed. “Yes! I’m wearing his wife’s clothes!” and we all had a good laugh. We instantly bonded and I learned more about how people with hemophilia can come here for free care.
Dr. Bari heard my story, and then shared that we both had a common inspiration point: me, with the birth of my son in 1987, and he in 1987 as well, when he first conceived the idea for such a hospital.
After our meeting I met a lovely elder man with VWD, who is in need of factor. He has had a bone that leaks pus constantly despite multiple operations. I’ll follow up with staff to learn more if Project SHARE can help. Despite all the help and dedicated physicians, Pakistan still faces so many restrictions and limitations medically.
After our tour here, we drove in the crazy, no-lane-awareness of Karachi traffic. It’s like being flushed through a convoluted traffic pipe as we dodge auto-rickshaws, donkey carts, hundreds of motorbikes, cars and trucks, horns blasting, all with some sort of preternatural grace. I never once saw a car get so much as scratched and yet car and motorbike come within mere inches of hitting constantly. I long since lost my reflex to slam my foot on the floor or grab the dash. You just go with it!
The NIBD (National Institute of Blood Disease & Bone Marrow Transplantation ) was founded by my friend Dr. Tahir Shamsi. It’s an 80 bed hospital in the heart of Karachi. It specialized in hematology, bone marrow transplantation and surgical specialties. It’s the only tertiary care and teaching institute in the country exclusively dedicated to provide comprehensive diagnosis and management of patients suffering from blood disorders. In fact, Tahir pioneered BMT in Pakistan and NIBD has performed more than 700 BMT. I can say I truly know some of the best people in medicine in the world!
Dr. Tahir Shamsi, founder NIBD
I can also say that I was present back in 2001 I think, when Tahir shared this dream with me: to create such a hospital. I had invited him to a medical symposium my company funded in Nepal, as a guest speaker. After the program, we sat in the lobby of the hotel, having tea, on the floor (why, I forget!) and he grabbed a napkin and sketched out a logo and an idea. I so wish I had that napkin today, because I saw vision in action. A dream became a vision which became a goal which gave birth to a strategy. The vision compelled others to help, and Tahir was on his way. Today I entered this institute, amazed at the number of patients, the 400 staff, the multiple floors, the progress, the research, the teaching.
I had the honor to meet three of Tahir’s interns, all hematologists, who want to one day go back to their home cities, and start hemophilia care there, particularly in Balochistan, where patients are largely unidentified. We chatted about steps to ensure this happens, and of course, how to make a dream come true! The men were a bit reserved but as we got talking, because more animated and spoke with more conviction. It was exciting to witness! I want to help them see this through, because their passion should be fed like a flame, and not allowed to die for lack of nurturing.
When the tour was over, around 5:30, I looked forward to going back and relaxing. But no such thing! After picking up Tahir’s sweet mother—I adore her—we headed with the entire family to Kolachi, a breathtaking wooden framed restaurant on the Arabian Sea. It was lit up with strings of white lights, draped like the scarves the women wear here, around the neck of the roof. Sea doves flitted across the top of the water, temporarily hitting the refection of the lights, making them glow for a moment. Roti, spinach and all sorts of things. I’m not a foodie, so I can’t report on anything I ate other than Pakistani food is excellent!


 “No longer can anyone say that someone with hemophilia can’t climb Everest, Vinson or reach any dream, as long as they have with proper treatment, training and medical care. By standing on these Seven Summits, I hope to show what is possible. I hope by holding the Save One Life banner on each summit we can show the world that only 25% of people living with hemophilia even have access to adequate treatment to chase dreams. Let’s help everyone aim for their dreams by helping to raise $16,050—the height of Vinson— for our scholarships!”
“No longer can anyone say that someone with hemophilia can’t climb Everest, Vinson or reach any dream, as long as they have with proper treatment, training and medical care. By standing on these Seven Summits, I hope to show what is possible. I hope by holding the Save One Life banner on each summit we can show the world that only 25% of people living with hemophilia even have access to adequate treatment to chase dreams. Let’s help everyone aim for their dreams by helping to raise $16,050—the height of Vinson— for our scholarships!”