Adoptions: Bringing Hudson Home
 |
| John “Poppy” Parler holding little girl at orphanage |
On Sunday,
May 7, after a 24-hour delay and a 14-hour flight from Beijing to Washington,
D.C., I stepped off United flight 808 at 7:15 PM with my third son, Dallas, and
my 14th grandchild – a six-year-old boy with severe hemophilia A –
who his entire life had been known as Chang Wang Le. Knowing we would pass
through immigration and, with one more official stamp on his paperwork, his
name would legally change to Hudson John Le Parler, we would then experience
the long-anticipated meeting with his forever mother, April, and his forever
brother and two sisters. While that moment would mark the end of a trip that
had begun for me over two weeks earlier, it was the culmination of a journey
which had begun, quite unexpectedly, over a year ago.
2016, at the Michigan Hemophilia Foundation’s annual Springfest Family
Education Weekend I met Shari Luckey, the Advocacy and Outreach Coordinator for
the Michigan chapter, and mother of a boy with hemophilia she adopted from
China in 2010. She shared her story and I
asked her about the need, process and challenges of that type of adoption. Her
answers were filled with passion for helping children with hemophilia overseas get
adopted.
shared her passion with me, I kept thinking of my son, Dallas, and his wife,
April. Dallas is the third of my five kids; he does not have hemophilia, unlike
his two brothers with severe hemophilia A. So he’s no stranger to the
challenges of living with hemophilia. Additionally, he and April always had a family
plan to have four biological children and then adopt one more child, or possibly
two more children. Since they already had three kids at the time, I thought it
might be interesting to pass the information Shari was providing along to them
in case they might have an interest four or five years down the road.
returning home, I did just that, and promptly forgot all about it. A month
later, much to my shock, in a casual conversation, Dallas mentioned to me that
they had applied to an adoption agency with the intent of pursuing adopting one
of the numerous boys available in China’s orphanage system. And so began their
journey to “Bring Hudson Home.”
there were reams of paperwork, financial disclosures, personal interviews, home
studies, and fees, followed by more reams of paperwork. It was sluggish and
tedious and I kept waiting for the word that they had decided to put the entire
process on hold. But that word never came. They persevered and plowed through
all of the bureaucratic red tape that inevitably accompanies an international
adoption, and – as they did – they began to accumulate a growing following on
the Facebook page they had established to document their journey. Those
followers came from every conceivable interlocking network of relationships;
their family and friends, friends of family, co-workers, their family’s
co-workers, other adoptive parents, the hemophilia community – the circle of
relationships expanded until nearly 800
people were following along every step of the way!
2016, the kids received some very
unexpected news—they were expecting their fourth biological child! I was
certain that this would put their journey on hold. I was wrong. By that time,
their adoptive son had already been identified, they knew his story, they were
aware that, in addition to his hemophilia, he had a congenital heart defect
from birth, and any thought of suspending the process would, in their minds, be
abandoning this little boy. So they persisted.
significant challenges faced Dallas and April. One – which had been there from
the start – was the cost of the adoption; approximately $35,000. The other
– April would be due with their next
child less than two months before the anticipated travel to China to finalize
the process, and unable to make the trip. That’s where I was summoned off the
sidelines and thrust into the middle of the process. The kids asked me to
accompany Dallas to China to provide logistical travel assistance and to help
during the two weeks he would have his newly adopted son with him, traveling
domestically, attending hearings and meetings and living in hotel rooms – with
a six year old who spoke no English. I could not refuse.
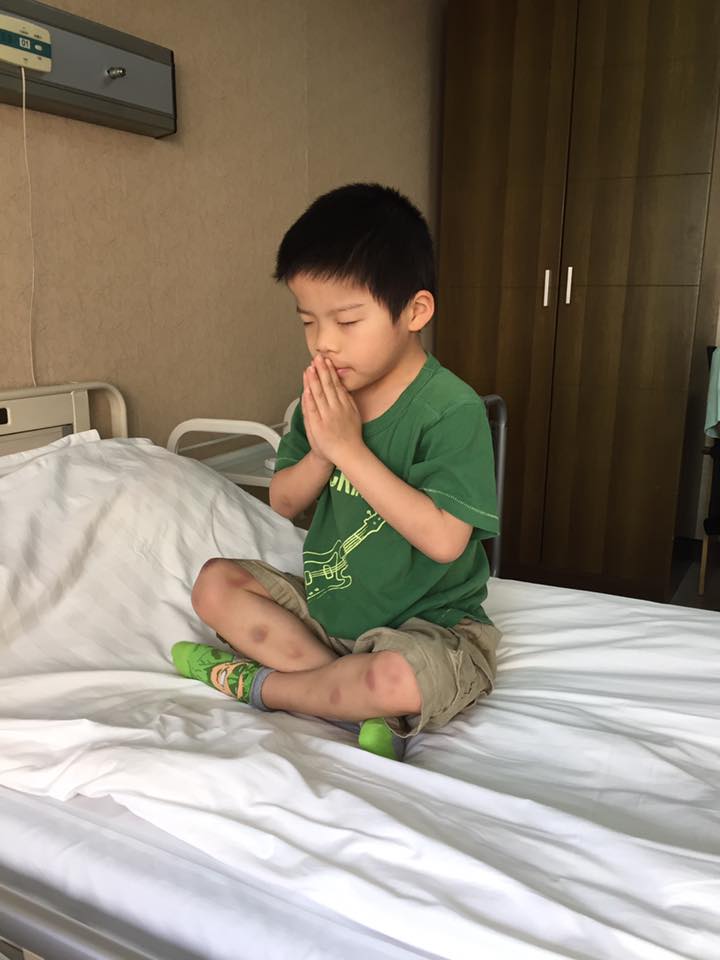 |
| Praying for a good infusion! |
As our
departure date in mid-April, the financial challenge remained unresolved. While
the kids, through their own efforts and the generosity of others, had already
spent $25,000 on the process, one significant financial obligation remained: a
mandatory $6,000 contribution to the orphanage required by the Chinese
government. I posted about the orphanage donation on the Facebook page
dedicated to Hudson. Within 5 days, that network of interested people generously,
graciously provided every last dime needed to provide that donation!
21, Dallas and I embarked on our trip to Bring Hudson Home. Words are
inadequate to convey all we experienced over the ensuing two weeks, first in
Nanjing and then in Guangzhou.
second full day in China, we were driven to a building where domestic marriages
and international adoptions are officially transacted. For Dallas, it is known
by adoptive parents as “Gotcha Day”; the day the parents are given custody of
their adoptive child. I had the incredible privilege, not only of meeting my
newest grandchild for the first time, but also of watching my own son’s face as
he met their son for the first time after such a grueling process! It was an
experience filled with absolute, unbridled joy!
 |
| Infusion time! |
week, we toured the orphanage where Hudson had lived, and where he received his
bi-weekly factor infusions. We had been pleasantly surprised to learn just
weeks before our departure that he had been receiving these infusions for the past year.
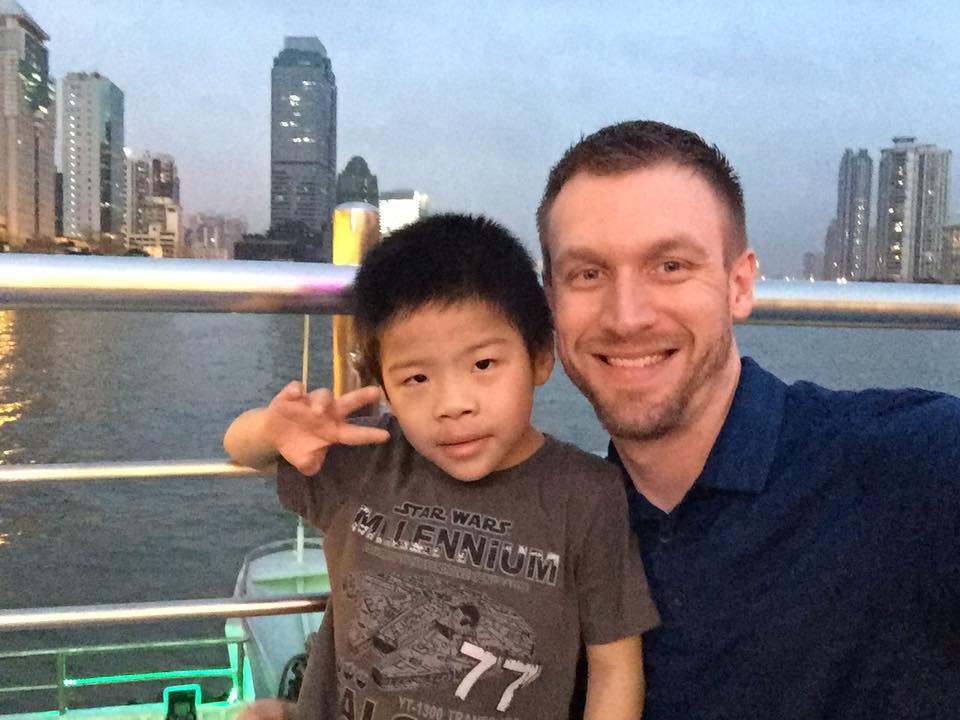 |
| Dallas Parler and Hudson |
But nothing prepared
us for what we witnessed that day. Hudson was receiving bi-weekly infusions
with a standard factor product, about one
half of the manufacturer’s recommended dosing for a boy his size. It was a
stark reminder that Hudson – and every other boy with hemophilia in the
orphanage system – was woefully under-treated.
understand fully what we witnessed on that tour, it’s important to understand
the context in which China’s orphanages now operate. Twenty years ago, this
same orphanage would have been filled with healthy little girls, primarily
because of the cultural preference for boys to carry on the family name coupled
with, at the time, China’s one-child policy. Today, however, thanks to the
repeal of that policy combined with a variety of other factors, in the same
orphanage (and in orphanages all across China) 98% of all orphans are children suffering from a wide variety of mental or
physical disabilities, or very expensive medical conditions for which their
birth family has no means of providing.
 |
| Proud Poppy! John and newest grandson Hudson |
attempt to deal with this changing demographic of abandoned children, China has
created “baby hatches” – tiny buildings at the entrance of every orphanage
where parents can safely abandon children they either do not want, or for whom
they simply cannot care. In 2016, one baby hatch in the Shandong province
received 106 children in the first eleven days it was open – all with disabilities or medical
conditions! Among those being turned over to the orphanages are a growing
number of boys who have hemophilia.
through Hudson’s orphanage, we entered a room with about 50 children under age
2. It was a large room with a soft mat floor, across which were scattered
little clusters of nannies surrounded by children. The nannies were doing their
best to hold children in turn and provide some semblance of attention and
stimulation. In spite of their best efforts, there were little ones left to
themselves, some entertaining themselves with well-used toys, others crying
inconsolably, and some just lying staring into whatever abyss their little
minds had created as a refuge for themselves. It was one little girl in that
state who caught my attention, and whom I picked up and held for nearly 20
minutes while she simply stared up into my face. That image – compounded by the
nearly 1 million abandoned children that live in China’s orphanage
system today – is one that will last a lifetime. While Dallas and I were
ecstatic at the thought of his and April’s ability to provide a family, a home,
security, love, hope and a future for Hudson, the reality that surrounded us in
that moment was crushing. It was a heart-breaking, gut-wrenching experience!
remainder of our trip was filled with much waiting, vitally important
processing of paperwork and great anticipation for heading home. When we
finally left Guangzhou for Beijing on our return, we were full of adrenalin and
excitement. Then the one flight we were to connect with to return from Beijing
to DC was – after 7 hours of waiting at the gate – cancelled. But 24 hours
later, we boarded that final, seemingly endless flight and we – finally – Brought
Hudson Home!
 |
| Parler Family with newest son |
The
beautiful, exciting sight of Hudson meeting the rest of his Forever Family is one
I will never forget. It marked the end of one journey and one trip, but it
marked the beginning of a life-long journey for Hudson. I have no idea what
that journey will hold for him, but I do know that because of the compassion
and sacrifice of my kids and their family, and the generosity of so many
strangers who were moved to help, he will be able to face a life where neither his
limitations nor opportunities will be defined by being born with severe hemophilia.
the 21st little boy from China with hemophilia in the past seven
years – that we know of – to be given the opportunity to become part of a
family here in America. Here, they will have access to the best treatment for
hemophilia in the world. And yet, there are more remaining in China – and other
countries around the world – desperately waiting for that same hope to become
their reality.
about international adoptions and hemophilia, download our PEN article: “Overseas Adoption: A Child with Hemophilia is Waiting”