See how they solved their pre-teen’s biggest treatment challenges
This is a paid public announcement from Sanofi and does not constitute an endorsement of products or services. When you click on the links in this blog entry, you will be directed to a Sanofi website. LA Kelley Communications always advises you to be a savvy consumer when contacting any company; do not reveal identifying information against your will.
You’re no stranger to drama: Adapting to changing needs, schedules, and even personalities is part of being a caregiver to pre-teens and early teens. As your child’s needs are changing, their treatment routine may need to change with them.
As your child flexes their independence and becomes more socially active, fitting multiple treatments into an already busy schedule may be a challenge, leading to missed treatments. They also may be more physically active than they have been in the past, and need sustained protection to feel confident playing sports or digging into their latest passion.
Luckily, this “awkward phase” of your child’s treatment journey is a transitional one. To help you through it, caregivers from the ALTUVIIIO® [antihemophilic factor (recombinant), Fc-VWF-XTEN fusion protein-ehtl] Peer community have shared their stories, insights, and advice, amplifying what you may have learned through your local hemophilia community.
Keep reading to learn how Natalie, Tara, and Allison helped their pre-teens build the right infusion routine, understand their treatment, and plan infusions around their family’s busy lives.
NATALIE & SAMUEL

“If anything about their current treatment is not working, from bleed protection to infusion schedules, you should always be confident in advocating for their care.” —Natalie
Letting life take center stage
Natalie and Samuel, 14
Years ago, when Samuel’s mom Natalie couldn’t find his vein during an infusion, the family’s trip to their favorite amusement park turned into a fun-filled visit to an infusion center instead.
Living with his family of 7, including a brother who also has hemophilia, Samuel remembers his former treatment infusion schedule was often “tricky.” Finding time to infuse with their already busy schedules had an unintended impact on the whole family.
When they considered a different treatment option for Samuel, Natalie was clear about what they needed as a family: “He had to be well-protected against bleeds, and we knew Samuel preferred infusions. And, of course, he wants to stay busy, so minimizing how frequently he infused was a significant consideration, too.”
His hematologist mentioned once-weekly ALTUVIIIO® and they switched in 2023. Since switching, his trough levels are around 15% on Day 7. For Samuel, stability is better than any rollercoaster ride saying, “I feel really good about my bleed protection and haven’t had any bleeds while on ALTUVIIIO.”
Check out Natalie & Samuel’s story
TARA & JACK

“We let Jack have the final say about switching. I provide my opinion, but he must also learn to manage his treatments independently.” —Tara
Keeping up with his physical activity
Tara and Jack, 14
“When Jack was first diagnosed, he was treated on demand. He fought really hard, so he missed treatments because it was nearly impossible,” remembers Jack’s mom Tara. Luckily, as he got older and decided he wanted to play sports, Jack began to understand the role his treatment played and became more cooperative.
However, when he turned 13, the family experienced new challenges. As a runner, he was starting to have some knee and ankle pain. And, as he was treating with factor mimetic, breakthrough bleeds required that they supplement with factor. His treatments were not just complex, but also difficult to track.
In 2024, Tara and Jack switched to ALTUVIIIO on his doctor’s recommendation. Since then, Jack has had less pain in his joints, and hasn’t experienced any joint bleeds or needed extra doses.
Check out Tara & Jack’s story.
ALLISION & EMILIO

“Whether you live with hemophilia or care for someone who does, we want you to know that you can do this.” —Allison
Taking control with the right treatment
Allison & Emilio, 16
From the beginning, Emilio wanted to be a part of managing his own treatment. He surprised his parents by asking to push his medicine and remove the needle himself at 10 years old. Then, after attending camp for children with bleeding disorders for several years, Emilio started self-infusing at age 13.
An avid swimmer who plays basketball, Emilio balances practices and games with school and time with friends. His previous treatment routine often meant infusing twice a week—or more, if he experienced a bleed—which overwhelmed his already full schedule.
Allison first heard about ALTUVIIIO at a hemophilia conference, and hoped it might allow Emilio to infuse once weekly. He started ALTUVIIIO in 2023 and hasn’t experienced any bleeds since. His trough levels are around 6.8% on Day 7.
Today, he volunteers at camp, helping younger kids learn how to infuse. “My hope is that he continues to grow more independent,” Allison says. “I want him to know he can achieve anything he sets his mind to.”
Check out Allison & Emilio’s story
Patient stories reflect the real-life experiences of persons diagnosed with hemophilia who have been prescribed ALTUVIIIO. However, individual experiences may vary. Patient stories are not necessarily representative of what another person using ALTUVIIIO may experience. Peer stories are based on data collected April 2026.
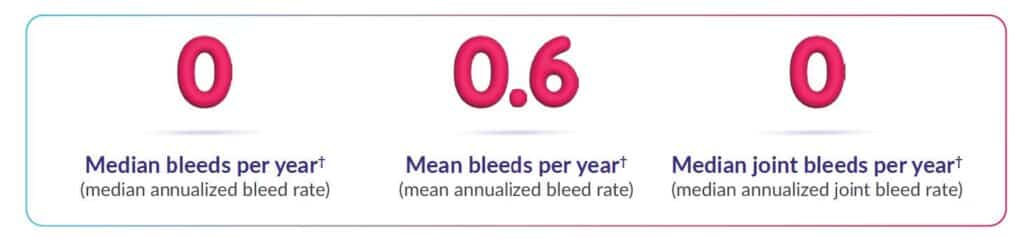
Here’s the most important information you need to know about ALTUVIIIO: Proven bleed protection with ALTUVIIIO prophylaxis
ALTUVIIIO was studied in XTEND-1 over 1 year, in 159 adults and adolescents (aged 12 and older) with severe hemophilia
– The trial included 158 male and 1 female participants
– Group 1 (133 people) switched from prior prophylaxis therapy to ALTUVIIIO prophylaxis, and efficacy was evaluated in 128 of these patients (including 1 female patient)
– Group 2 (26 people) switched from prior on-demand therapy to ALUTVIIIO on demand for 52 weeks, and then to ALTUVIIIO prophylaxis for 26 weeks
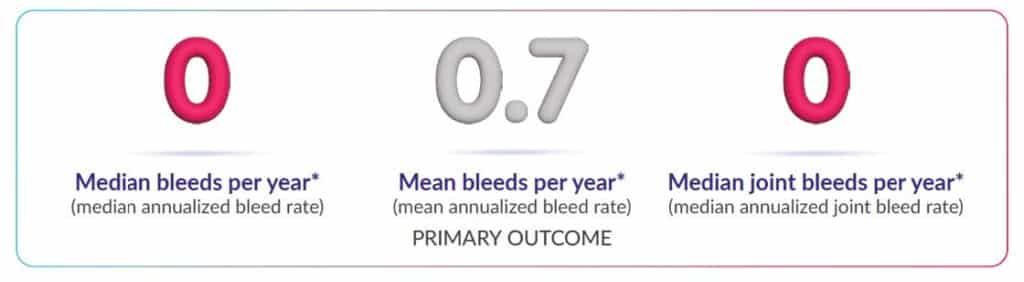
Kids can experience proven bleed protection with ALTUVIIIO prophylaxis*
ALTUVIIIO was studied over 1 year in the XTEND-Kids study
74 previously treated male children under 12 years of age who switched to ALTUVIIIO:
- 36 children aged 6 to under 12 years
- 38 children under the age of 6
- Efficacy was evaluated in 72 of these children
The primary goal of the XTEND-Kids study was to determine whether or not children under 12 years of age developed inhibitors to ALTUVIIIO.
- 0 inhibitors detected in the 74 children
- Although no inhibitors were found in clinical studies, inhibitors have occurred with ALTUVIIIO in the postmarketing setting
In 233 people across the clinical studies‡:
• 15% experienced headache (35 people)
• 13% experienced joint pain (31 people)
• 4% experienced fever (10 people)
• 4% experienced pain in extremities (10 people)
• 4% experienced back pain (9 people)
• 3% experienced vomiting (7 people)
Learn about our safety profile
*Efficacy was evaluated in 72 children in the XTEND-Kids study.
†Data based on treated bleeds.
‡Included participants of the XTEND-1 and XTEND-Kids studies.
Learn about our safety profile
*Efficacy was evaluated in 72 children in the XTEND-Kids study.
†Data based on treated bleeds.
‡Included participants of the XTEND-1 and XTEND-Kids studies.
INDICATION
ALTUVIIIO® [antihemophilic factor (recombinant), Fc-VWF-XTEN fusion protein-ehtl] is an injectable medicine that is used to control and reduce the number of bleeding episodes in people with hemophilia A (congenitalFactor VIII deficiency).
Your healthcare provider may give you ALTUVIIIO when you have surgery.
IMPORTANT SAFETY INFORMATION
What is the most important information I need to know about ALTUVIIIO?
Do not attempt to give yourself an injection unless you have been taught how by your healthcare provider or hemophilia center. You must carefully follow your healthcare provider’s instructions regarding the dose and schedule for injecting ALTUVIIIO so that your treatment will work best for you.
Who should not use ALTUVIIIO?
You should not use ALTUVIIIO if you have had an allergic reaction to it in the past.
What should I tell my healthcare provider before using ALTUVIIIO?
Tell your healthcare provider if you have had any medical problems, take any medications, including prescription and non-prescription medicines, supplements, or herbal medicines, are breastfeeding, or are pregnant or planning to become pregnant.
What are the possible side effects of ALTUVIIIO?
You can have an allergic reaction to ALTUVIIIO. Call your healthcare provider or emergency department right away if you have any of the following symptoms: difficulty breathing, chest tightness, swelling of the face, rash, or hives.
Your body can also make antibodies called “inhibitors” against ALTUVIIIO. This can stop ALTUVIIIO from working properly. Your healthcare provider may give you blood tests to check for inhibitors.
The common side effects of ALTUVIIIO are headache and joint pain.
These are not the only possible side effects of ALTUVIIIO. Tell your healthcare provider about any side effect that bothers you or does not go away.
Please see full Prescribing Information.
Please consult your healthcare professional if you have any questions about your health or treatment.
© 2026 Sanofi. All rights reserved. ALTUVIIIO and Sanofi are registered trademarks of Sanofi or an affiliate.
MAT-US-2603389-v1.0-04/2026