The Not-So-Royal Disease
It’s March—Bleeding Disorder Awareness Month!

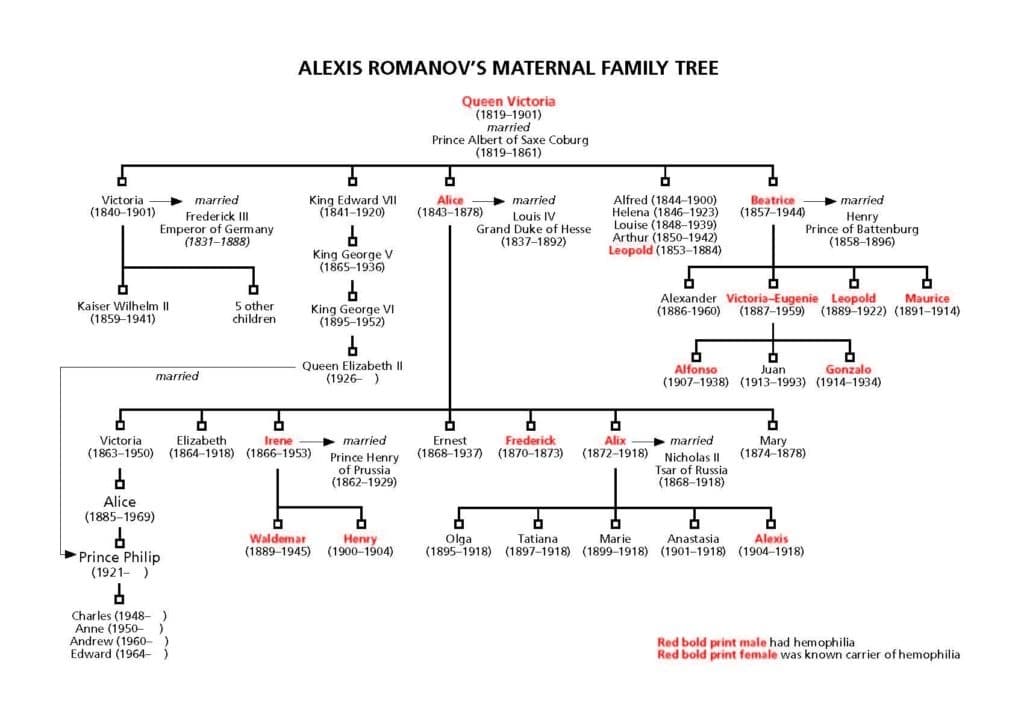
For most people, hemophilia is an obscure disorder, associated with royalty. In fact, it is erroneously dubbed “The Royal Disease.” But this is a fallacy. It is true that hemophilia was once linked to the royal families of Europe, thanks to the most famous carrier of the hemophilia gene: Queen Victoria of England. She was, until Queen Elizabeth II, who passed away at age 96 in 2022, surpassed her, the longest ruling monarch in history, at 63 years and 216 days. Queen Victoria, a known carrier of factor IX deficiency, also called hemophilia B, was Queen Elizabeth II’s great-great-grandmother. Queen Elizabeth II was the mother of the current king, King Charles II, father of William and Harry.
Queen Victoria had nine children; one son, Leopold, had hemophilia. He passed the carrier gene to his daughter Alice. Descendants of Victoria would marry into the royal families of Russia, Spain, and Germany, and have children with hemophilia. One famous child from this lineage was Alexei, Prince of Russia, son of Tsar Nicolas II. This royal family was killed by the Bolsheviks on July 18,1918.
Victoria and her descendants truly put hemophilia on the map. And that’s where we get the moniker “Royal Disease.”
Hemophilia is no longer known to be present in any European royal family. Since Queen Elizabeth II had no hemophilia in her direct lineage, neither Charles nor his sons, William and Harry, have hemophilia or were ever at risk of inheriting it. We are happy none of them have hemophilia, but even if they did, with the excellent treatments we have today, it would not interfere much with any royal duties.
Hemophilia may still be associated with royalty but in truth, anyone can get hemophilia—rich or poor, famous or unknown.
Order a copy of Alexis: The Prince Who Had Hemophilia to learn more!