Land of One Thousand Hills… and Challenges Part I

twentieth anniversary of the start of the genocide, April 1994. I recall
vividly watching my TV each day, holding my newborn, Mary, and helplessly
comparing her blessed life with the sufferings of the refugees in Goma, and
those trapped in their villages and in the capital, Kigali. The genocide went
on for three months while the world mostly watched, indifferent, unbelieving,
and immobile. It was then and there that I resolved to do something to help those with hemophilia in other countries. Later, Save One Life was born.
central Africa, about the size of my home state, Massachusetts. Nearly half of
its 11 million people live in Kigali, the capital. Colonized by first the
Germans, then the Belgians after World War I, it is an independent state now
where English and Kinyarwanda are spoken. About 95% of the population is
declared Christian.

The current GDP (“income”) of Rwanda is about $15.7 billion, which ranks it at #141 in the
world. Average income is about $ 600 a year. And about 45% of the population
lives below the poverty line.
only tea and coffee being exported. Thanks to the wild mountain gorilla
population, tourism is the number one industry, with farming a close second.

My first impressions were all positive of this enchanting African land. I looked
at the stunningly beautiful pastoral vista: rolling hills, tiered like a cake
with green frosting, all farms and crops. Patched-worked in were squares of
other crops: banana trees, sugar cane, pineapple, sorghum. And everywhere
people walk, balancing great loads on their heads. Even the children: their
faces disappear under great loads of bamboo, until they resemble huge bails of
greenery with legs. Or small children struggle to haul water jugs back to their
homes. Infants are wrapped and tied onto their mother’s backs, asleep. Women
work hard here. Men push bicycles up hill, with a towering 50-lb sack of
potatoes or yams. The children wave at me and say “Allo!” A huge field in the
foothills is dotted with colorfully clothed Rwandans chopping and turning the
earth with hoes; backbreaking work.
will cover the visits to the Genocide Museum, churches and then the Mountain
Gorillas. Because to know Rwanda, you must know more about the Genocide, and its natural wonders which attract people from around the world.

is a young hematologist and the only hematologist in a country of 11 million.
He had just recently returned from training in South Africa. His daughters
Alegra and Farley were charming and we enjoyed conversing with them.

patient-centric organization after her other son Jose died. After knowing her
and working with her for several years, I asked her to accompany me on this
trip to create a bridge between the two countries. To me, it’s silly to have
African nations reaching out to the West constantly, and for us to help
unilaterally, when Africans can share and should share with one another.
Maureen would have much wisdom and experience to share with the patient group the next day.
works, to meet with many doctors of different disciplines. I gave a talk about
the need for leadership in starting a hemophilia foundation and also in
changing history—here, to create a hemophilia program that addresses problems medically and socially.
donation from the World Federation of Hemophilia was received! December 2012!

is deeply involved, where health expenditures are 10.8% of GDP, placing Rwanda at 17th in the
world, where HIV prevalence is 3%, one of the lowest rates in Africa.

district hospitals, and 45,000 community health workers providing care are the
village level, Rwanda has created a system to bring health care to both its
urban and rural populations. Yet, life expectancy is only 64 years (and lower
for men).

population of 11 million, there should be about 400-500 with hemophilia. Yet
only 27 have been identified. Dr. Fabien showed us the blood lab, where a one
humble machine stood. Rwanda needs a proper diagnostic facility, in order to
test those with factor VII and factor IX, those with inhibitors or von
Willebrand disease.
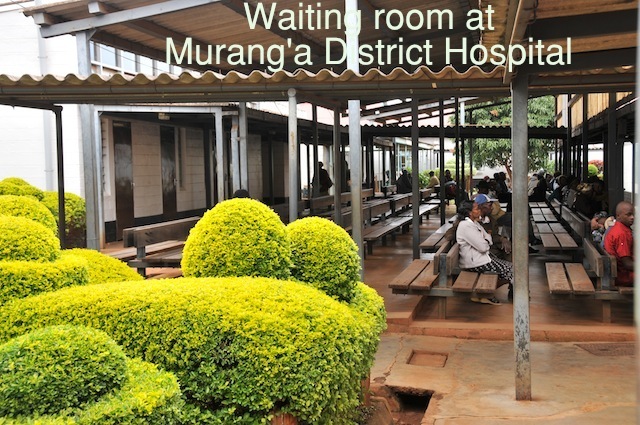
The pediatric wards were bright and cheery, with beautiful beds (so remarkable not to see chipped paint, stained walls, overcrowded facilities) and clean floors and walkways.
lunch together, and then waited for the parents/patients to show up at 2 pm for
our first meeting of the Rwanda Federation of Hemophilia. This group was formed
in February 2013, but in actuality, nothing has been implemented or become
official. The group is not registered as a proper nonprofit with the
government, which then prevents it from participating with the WFH and
receiving the resources it needs and deserves. Our mission is to get the group
together, sort out why it has not been registered, get it registered, and get
it moving, according to the tenets of my book, Success as a Hemophilia Leader.

included: Emmanuel, Alyos, and Sylvestre, all fathers of children with
hemophilia; young people Fred and Prince, brothers, and their mother. Prince, age 15, was on
crutches and needs to have x-rays to determine if surgery is possible to fix
his patella, which was knocked loose during an accident. Dr. Fabien, in spite
of all the work he has to do, had done his part and got this community
together, bless him. We met for over an hour, talking about what needs to get
done to get this new initiative moving. We ordered soft drinks and African tea
for everyone. Maureen’s lecture on what she has accomplished with JMHS was
superb and opened their eyes to possibilities—what they as a group of patients
and parents can accomplish. As an African, she can communicate with them as I
cannot; she has that credibility that I don’t.
constitution (It needs reviewing as it’s been a year); temporary elections were
needed today, now, to get leaders in place (done!); priorities need to be
established (blood diagnostic lab and registering the society). We accomplished
all that. Fred, only age 21, took the Minutes. We were having our first proper
meeting.
that needs to be done.
other guests. A pediatrician, the Minister of Health understood about hemophilia. I showed her photos on my laptops of some severe cases. And then we cut to the chase.

offers health care for all individuals to access medical services, currently
95% of the population have access to insurance (current annual insurance cost
is approximately $5). Medicine is sold at pharmacies, and patients get reimbursed
about 80% through the government. Could this be done with factor?
It would overwhelm the system and is too expensive. And honestly, I thought,
asking parents and patients to pay just 20% of the costs would wipe them out.
So there is no easy solution for treatment of hemophilia in Rwanda. Yet,
Barbados, a small Caribbean country, purchases factor; Honduras, one of the
poorest countries in the Western Hemisphere, purchases factor. How can we move
other countries in the same direction?
structure fortified by the patients, families and physicians (the Rwanda
Federation of Hemophilia; it takes help from the outside world (the WFH and
entities like us and the JMHS-K); and it takes time. And over time, Rwanda will
achieve self-sufficiency.

unbreakable Rwandan spirit, to which we owe the survival and renewal of our
country…” Think of the victims as those with hemophilia, and you can parallel
that we will succeed one day in providing hemophilia care to a nation that has
already suffered enough.
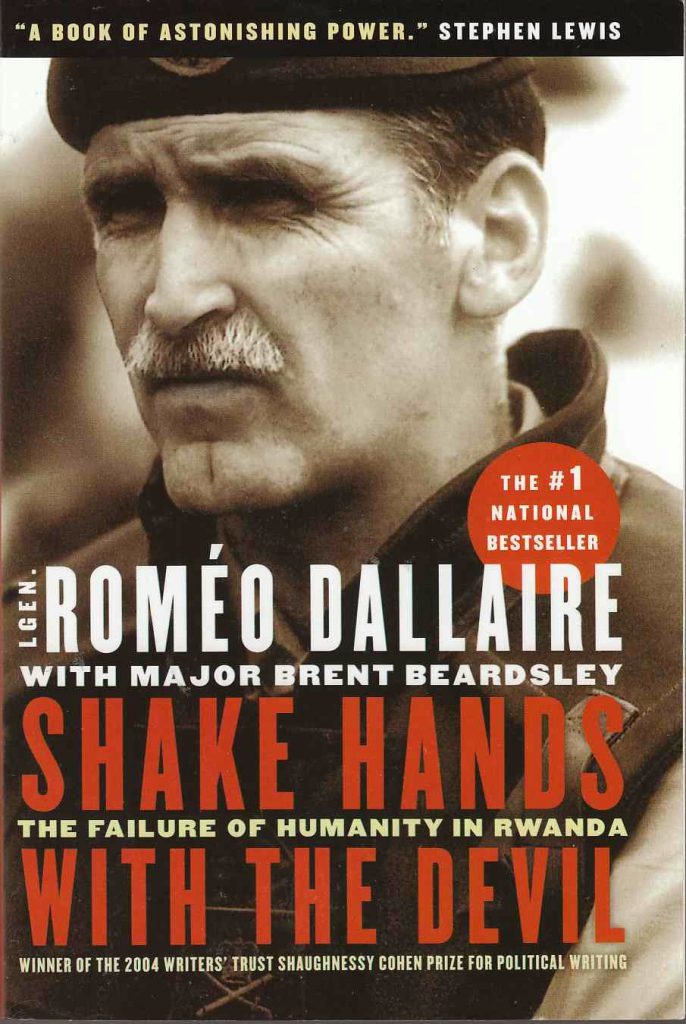 Dallaire was
Dallaire wasthe head of a UN peacekeeping mission during the 1994 civil war/genocide, in
which 800,000 Rwandans were slaughtered in three months. The book is not a
reporter’s eye-witness account of atrocities: it is a moment by moment, blow by
blow, insider leader’s view of the events leading up to the April 6, 1994
assassination of Rwanda’s president, the internal struggle to get the Arusha
Peace Accord finalized, the mobilizing of anti-governmental forces, the power
struggles between the Tutsi and Hutu tribes, the political players, and more. Dallaire
gives an exhaustively detailed account of what went on politically before
during and after the Genocide, both inside the country and globally; how the UN
on the ground reacted and the indifference of the world. It is a scathing
indictment of the bureaucratically hampered United Nations, the hesitant United
States and the self-serving Belgians. While the world watched, hundreds of
thousands of Tutsis and moderate Hutus were macheted and mutilated. How
Dallaire coped with the lack of resources, the suffering of his own troops,
constant gamesmanship of the players involved, death threats, lies from
politicians, and being surrounded by death and suffering of women and children
is nothing but heroic. He is a hero, and did his best. It is an exhausting book
to read in many ways, yet must-reading for anyone involved in charity work, war
time missions, history, the military, and huge international bodies like the
UN. So many lessons to be learned; Dallaire has done the world, history and
future citizens a vital service in providing this book. It should be a military/humanitarian
classic. God bless him. Five/five stars.