“My bones are older than me”
 |
| Prince, age 17 |
“My bones
are older than me,” lamented Prince, the handsome 17-year-old Rwandan with
hemophilia, who I had met previously three years ago when I first came to this
small, lush country. This night, Wednesday, June 14, I welcomed a few families
with hemophilia, who are the founders of the new Rwanda Federation of
Hemophilia. While all competent professionals, they still need some help in
getting their organization jumpstarted. Imagine living in a country that has no
factor, no hemophilia care, and is poor. Of the estimated 800 people with hemophilia here,
no more than 50 are identified.
are older than me,” lamented Prince, the handsome 17-year-old Rwandan with
hemophilia, who I had met previously three years ago when I first came to this
small, lush country. This night, Wednesday, June 14, I welcomed a few families
with hemophilia, who are the founders of the new Rwanda Federation of
Hemophilia. While all competent professionals, they still need some help in
getting their organization jumpstarted. Imagine living in a country that has no
factor, no hemophilia care, and is poor. Of the estimated 800 people with hemophilia here,
no more than 50 are identified.
But this is all about to change.
We gathered socially in the cool evening on the terrace at the famous Hôtel des Mille
Collines, dubbed “Hotel
Rwanda,” a safe haven during the brutal 1994 genocide, where the manager Paul Rusesabagina saved 1,268 Hutu and Tutsi refugees from the Interahamwe militia. (If you haven’t
seen the movie Hotel Rwanda, I urge you to rent it.) The Mille Collines is
a lovely hotel, and while I write this I hear a spry African ensemble playing traditional
music downstairs with chanting and upbeats that make you want to dance!
Collines, dubbed “Hotel
Rwanda,” a safe haven during the brutal 1994 genocide, where the manager Paul Rusesabagina saved 1,268 Hutu and Tutsi refugees from the Interahamwe militia. (If you haven’t
seen the movie Hotel Rwanda, I urge you to rent it.) The Mille Collines is
a lovely hotel, and while I write this I hear a spry African ensemble playing traditional
music downstairs with chanting and upbeats that make you want to dance!
 |
| Shady Sedhom, NNHF, listens to the patients |
Prince is rail
thin, and soft spoken, like all Rwandans. I’m glad he arrived first so I could
get caught up with him personally. When I saw him in 2014, I had arrived for
the first time in Rwanda to assist the new Federation. Prince was a stocky
14-year-old then. Now he was lean and taller, with chiseled features. When I
asked him how he was doing, he replied with a phrase that showed his desperate
plight, and poetic aptitude: “My bones are older than me. I have the bones of a
60-year-old, my doctor told me.” His right knee had given him a lot of trouble
three years ago; now the left one was. When was the last time he went to the clinic,
which was only 1 kilometer from his house? Not in years. Why? “Every time I go
they have no factor.”
thin, and soft spoken, like all Rwandans. I’m glad he arrived first so I could
get caught up with him personally. When I saw him in 2014, I had arrived for
the first time in Rwanda to assist the new Federation. Prince was a stocky
14-year-old then. Now he was lean and taller, with chiseled features. When I
asked him how he was doing, he replied with a phrase that showed his desperate
plight, and poetic aptitude: “My bones are older than me. I have the bones of a
60-year-old, my doctor told me.” His right knee had given him a lot of trouble
three years ago; now the left one was. When was the last time he went to the clinic,
which was only 1 kilometer from his house? Not in years. Why? “Every time I go
they have no factor.”
I’ve been
trying to keep Rwanda supplied with factor; indeed, we are the only ones who
give them factor. And that’s because they are not yet registered with the World
Federation of Hemophilia. Once they register, they will be eligible for much,
much more factor, perhaps regularly. Getting them registered, both with their
own government and then the WFH was my goal this trip.
trying to keep Rwanda supplied with factor; indeed, we are the only ones who
give them factor. And that’s because they are not yet registered with the World
Federation of Hemophilia. Once they register, they will be eligible for much,
much more factor, perhaps regularly. Getting them registered, both with their
own government and then the WFH was my goal this trip.
With me was
Mr. Shady Sedhom, a registered pharmacist and now program manager with the NovoNordisk Haemophilia Foundation, an incredible organization based in
Switzerland, that provides program expertise, management and funding for
hemophilia organizations globally. This was the second time I would work with
them, but the first time in person. We would give a half day workshop on
Thursday, June 15.
Mr. Shady Sedhom, a registered pharmacist and now program manager with the NovoNordisk Haemophilia Foundation, an incredible organization based in
Switzerland, that provides program expertise, management and funding for
hemophilia organizations globally. This was the second time I would work with
them, but the first time in person. We would give a half day workshop on
Thursday, June 15.
 |
| Benis’s knee |
But this
evening we were here to meet the board members, and hear their stories. I don’t
want to just give a lecture on how to run an organization: I want to know them,
as people, as families, as families with hemophilia, as blood brothers and
sisters in this amazing global family we have.
evening we were here to meet the board members, and hear their stories. I don’t
want to just give a lecture on how to run an organization: I want to know them,
as people, as families, as families with hemophilia, as blood brothers and
sisters in this amazing global family we have.
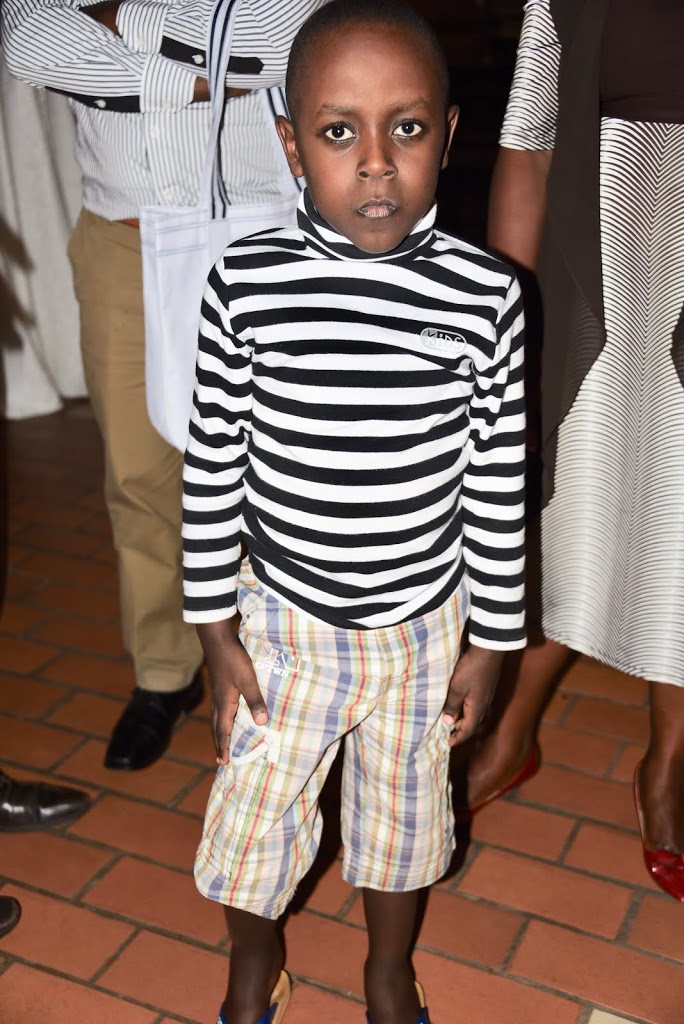
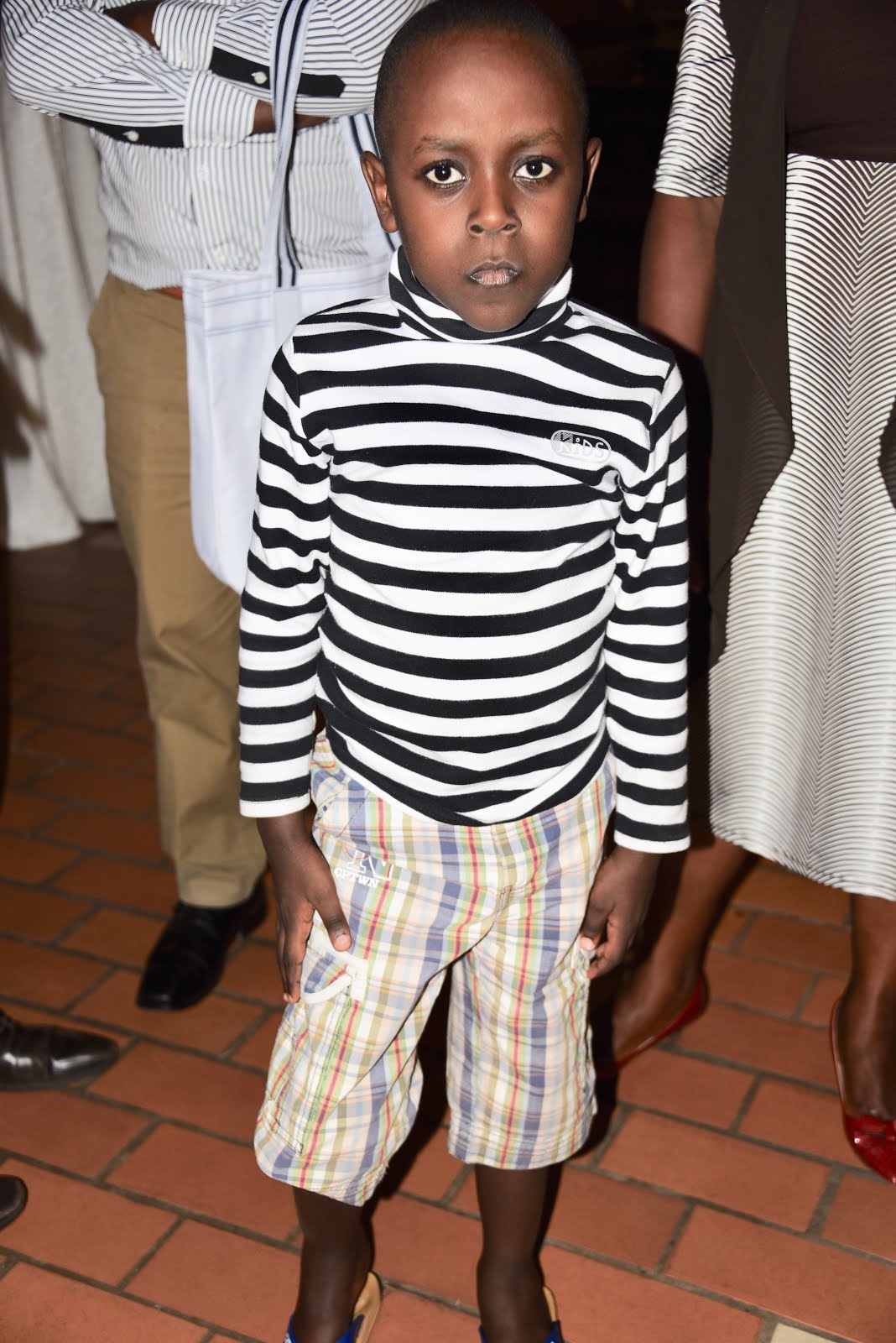 |
| Little Benis |
I met Vivine,
whose son Ness, now age 8, hemophilia B, had a headache as a toddler, and it
continued on. We listened in somber silence, as she continued. She took him to
the doctor, who tested him for malaria, but this was not it. They gave him a painkiller
and sent him home. The headache continued for two more days, getting worse. She
took him to the ER on a Friday night at the public hospital, but they said they
could not give him a CT scan because it was too late. Come back Monday! In a
culture used to respecting authority and not questioning the medics, Vivine’s
strong maternal instinct won out. She went to the King Faisal Hospital (a
private hospital), which would be prohibitively expensive. She went anyway that
night, and they diagnosed him with a head bleed! He got factor and this saved
his life. Her story highlighted the need for education among the country’s
doctors.
whose son Ness, now age 8, hemophilia B, had a headache as a toddler, and it
continued on. We listened in somber silence, as she continued. She took him to
the doctor, who tested him for malaria, but this was not it. They gave him a painkiller
and sent him home. The headache continued for two more days, getting worse. She
took him to the ER on a Friday night at the public hospital, but they said they
could not give him a CT scan because it was too late. Come back Monday! In a
culture used to respecting authority and not questioning the medics, Vivine’s
strong maternal instinct won out. She went to the King Faisal Hospital (a
private hospital), which would be prohibitively expensive. She went anyway that
night, and they diagnosed him with a head bleed! He got factor and this saved
his life. Her story highlighted the need for education among the country’s
doctors.
 |
| A fun evening with many shared stories |
We met
James, age 31, also hemophilia B, who was just diagnosed last year! James is a quiet man, lacking a few front teeth. Indeed, he had persistent dental
problems, with constant bleeding. When the doctors here could not figure out
what was causing this, he finally sent his blood to France to be tested, at
cost of $400! This is a ridiculous amount of money in a country where the average
annual household income is about $700. Especially since it could have been
diagnosed in neighboring Kenya.
James, age 31, also hemophilia B, who was just diagnosed last year! James is a quiet man, lacking a few front teeth. Indeed, he had persistent dental
problems, with constant bleeding. When the doctors here could not figure out
what was causing this, he finally sent his blood to France to be tested, at
cost of $400! This is a ridiculous amount of money in a country where the average
annual household income is about $700. Especially since it could have been
diagnosed in neighboring Kenya.
Sylvestre
has been my email pal for the past few months as we prepared for this visit. He
serves as Secretary of the RFH. Sylvestre is well known to us in the office
back home as he has requested factor for his son Virgil. Little Virgil,
squirming before me with all the energy of a four-year-old, wears glasses for
his still misaligned eyes. He was blind for 18 months after a coma, due to head
bleed as a two year old, but factor from Project SHARE saved his eyesight. Slowly,
Sylvestre told us, he is getting his eyesight back.
has been my email pal for the past few months as we prepared for this visit. He
serves as Secretary of the RFH. Sylvestre is well known to us in the office
back home as he has requested factor for his son Virgil. Little Virgil,
squirming before me with all the energy of a four-year-old, wears glasses for
his still misaligned eyes. He was blind for 18 months after a coma, due to head
bleed as a two year old, but factor from Project SHARE saved his eyesight. Slowly,
Sylvestre told us, he is getting his eyesight back.
Sylvestre
reminded me of how I got involved with Rwanda in the first place—I had actually
forgotten as we have accumulated so many stories working with so many countries.
A nurse named Tracy Kelly was volunteering in Rwanda about five years ago, and
met Sylvestre as he sought help for little Virgil. She contacted her hospital
back home, which eventually found us. We shipped factor over right away. And
when the crisis passed, I asked Sylvestre to consider founding a national
organization for those with hemophilia. Like many we have met, he agreed. And
here we were.
reminded me of how I got involved with Rwanda in the first place—I had actually
forgotten as we have accumulated so many stories working with so many countries.
A nurse named Tracy Kelly was volunteering in Rwanda about five years ago, and
met Sylvestre as he sought help for little Virgil. She contacted her hospital
back home, which eventually found us. We shipped factor over right away. And
when the crisis passed, I asked Sylvestre to consider founding a national
organization for those with hemophilia. Like many we have met, he agreed. And
here we were.
We finished our
juice drinks and tea and cakes, and then they dispersed into the soft night,
hopeful for the next day’s outcomes.
juice drinks and tea and cakes, and then they dispersed into the soft night,
hopeful for the next day’s outcomes.
 |
| Vivine adds a needs list |
The next day
was our workshop. Shady has a prepared slide deck, exercises and came equipped
with markers, post-its, posters. The attendees arrived early, prepared to work!
Besides the RFH we also had several doctors, which was a high point. Doctors in
developing countries have little free time. Most work at two hospitals and/or
have a private practice. They seem on call 24/7. To have them here was an
absolute honor. The day consisted first of a needs assessment, brainstorming
what Rwanda needs to have good hemophilia care. Each attendee wrote out ideas
on a post-it note then attached it to a poster, under one of four areas of
need. The post-its read: A comprehensive center, training, education of health
care workers and families, diagnosing suspected cases, outreach to find more
patients, public awareness to help find patients, and of course… more factor.
was our workshop. Shady has a prepared slide deck, exercises and came equipped
with markers, post-its, posters. The attendees arrived early, prepared to work!
Besides the RFH we also had several doctors, which was a high point. Doctors in
developing countries have little free time. Most work at two hospitals and/or
have a private practice. They seem on call 24/7. To have them here was an
absolute honor. The day consisted first of a needs assessment, brainstorming
what Rwanda needs to have good hemophilia care. Each attendee wrote out ideas
on a post-it note then attached it to a poster, under one of four areas of
need. The post-its read: A comprehensive center, training, education of health
care workers and families, diagnosing suspected cases, outreach to find more
patients, public awareness to help find patients, and of course… more factor.
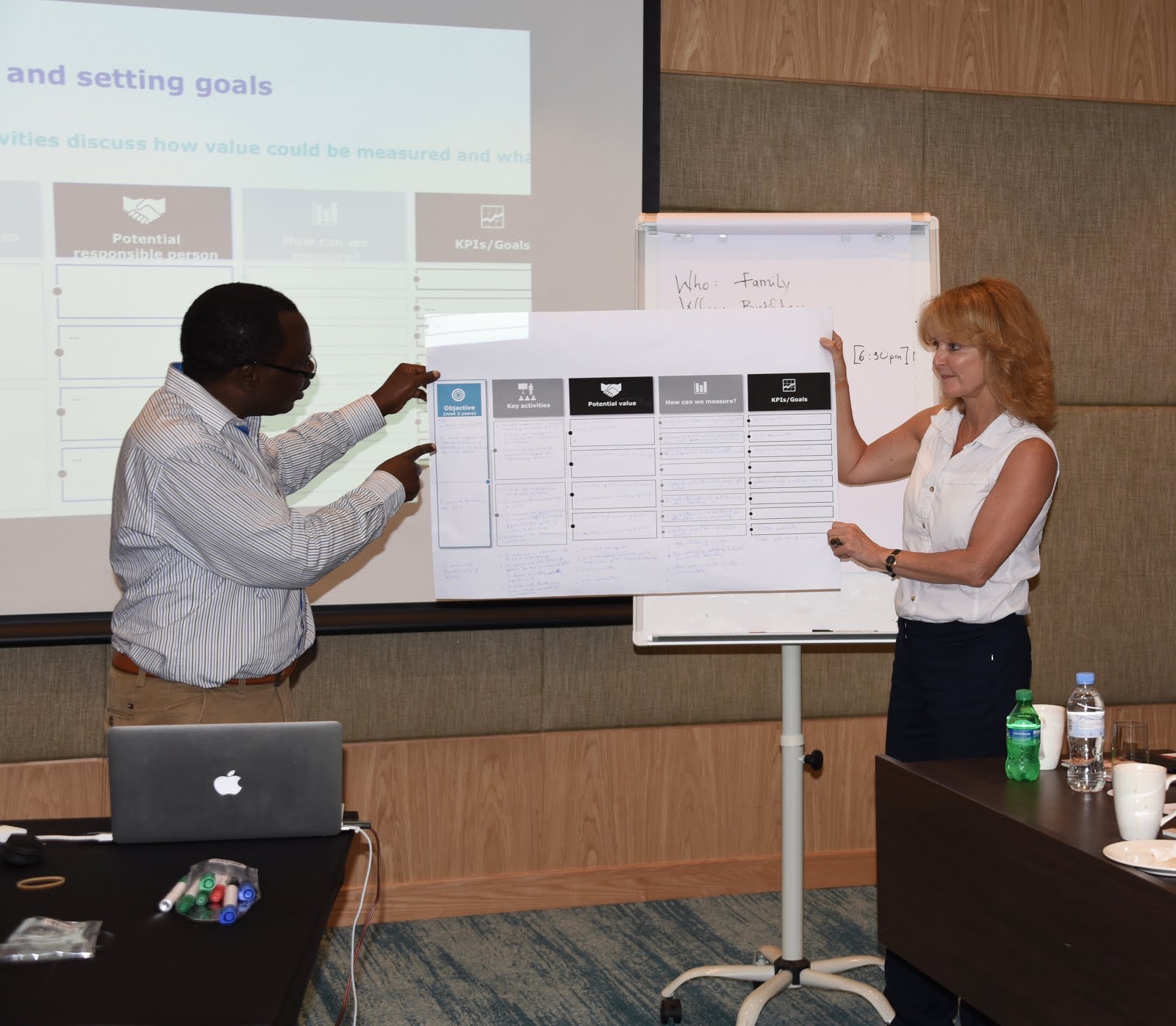
 |
| Laurie Kelley with patient at CHUK |
But the
greatest need was to register the RFH with the government. Until it becomes an
official, registered nonprofit, nothing much would happen. The WFH needs it
registered and accountable. Project SHARE will keep sending factor of course,
but we can only do so much. Shady said NHF is ready with funding for a project
to help meet these needs… after they get registered.
greatest need was to register the RFH with the government. Until it becomes an
official, registered nonprofit, nothing much would happen. The WFH needs it
registered and accountable. Project SHARE will keep sending factor of course,
but we can only do so much. Shady said NHF is ready with funding for a project
to help meet these needs… after they get registered.
And an
interesting phenomenon: learning how to challenge each other’s ideas. When
someone offered an idea, such as the most important need was to get more
factor, Shady and I challenged that. Spending your time securing factor is
urgent, especially when your child has a bleed. But allowing the registration
issue to languish means you will only get dribs and drabs of donated factor. Focusing
on registering now will open so many doors later. Short term pain for long term
gain. The RFH was learning now to priorities needs.
interesting phenomenon: learning how to challenge each other’s ideas. When
someone offered an idea, such as the most important need was to get more
factor, Shady and I challenged that. Spending your time securing factor is
urgent, especially when your child has a bleed. But allowing the registration
issue to languish means you will only get dribs and drabs of donated factor. Focusing
on registering now will open so many doors later. Short term pain for long term
gain. The RFH was learning now to priorities needs.
After this
we did goal setting, based on those needs. And then prioritizing those goals.
This took over an hour. Later, Shady asked the group to plan a birthday party,
as an exercise in planning a hemophilia event later on (like World Hemophilia
Day next April). It was a fun exercise to see who remembered what action item
was needed. And ironic: that very day, June 15, was Shady’s birthday! Unknown
to him I ordered a cake. And right after the birthday party exercise, we took a
break, and out came a cake with candles! It was fun to all join in and sing him
happy birthday. We thanked him for his dedication for spending his birthday working on Rwanda’s hemophilia future. Then we learned that we had another cause to celebrate: James’s wife had just given birth a few hours ago! But he stayed to complete the workshop with us. Such dedication!
After break
came Stakeholder Awareness, an exercise I’ve never done before so this was
educational for me. Even just learning who to identify who is influential and
how much they were influential—Prince offered the media, which was
brilliant—and others offered families, the public, the ministry of health and
more.
came Stakeholder Awareness, an exercise I’ve never done before so this was
educational for me. Even just learning who to identify who is influential and
how much they were influential—Prince offered the media, which was
brilliant—and others offered families, the public, the ministry of health and
more.
By the end
of the day we had the components of a strategic plan, with action items. It
will take many more meetings to hammer out the details but it was a powerful
five hours. Afterward, we dined outside in the night air and had a buffet
dinner together. Shady had to dash off to catch a flight but the rest of us
relaxed and shared our thoughts on this truly historic day.
of the day we had the components of a strategic plan, with action items. It
will take many more meetings to hammer out the details but it was a powerful
five hours. Afterward, we dined outside in the night air and had a buffet
dinner together. Shady had to dash off to catch a flight but the rest of us
relaxed and shared our thoughts on this truly historic day.
We planted
the seeds of growth, and now, it’s up to the Rwandans to take next steps on the
road to better hemophilia treatment care.
the seeds of growth, and now, it’s up to the Rwandans to take next steps on the
road to better hemophilia treatment care.


 And they
And theydeserve it and can do it. Rwanda spends more on healthcare per capita than most
African countries. The country is peaceful, functions well and has infrastructure.
It’s a small country, about the size of Massachusetts, my home state. Best of
all, it has interested and dedicated doctors. All ingredients of success.
There will
be challenges. I read a Rwandan proverb that says: If you are building a
house and a nail breaks, do you stop building, or do you change the nail? We don’t want them to ever stop building.
be challenges. I read a Rwandan proverb that says: If you are building a
house and a nail breaks, do you stop building, or do you change the nail? We don’t want them to ever stop building.
 |
| A reason to celebrate! |
My vision?
To see Rwanda join the WFH, and be present next year at the WFH Congress in
Scotland, where they will meet the world community, and their fellow Africans,
to learn, to share and to get the resources that so many others get. When they
join everyone else, they will then be able to determine their treatment and
destiny, and a whole generation of Rwandans will grow up free of the pain and
disabilities they suffer now.
To see Rwanda join the WFH, and be present next year at the WFH Congress in
Scotland, where they will meet the world community, and their fellow Africans,
to learn, to share and to get the resources that so many others get. When they
join everyone else, they will then be able to determine their treatment and
destiny, and a whole generation of Rwandans will grow up free of the pain and
disabilities they suffer now.
To see photos of the trip, go here.