We just wrapped up a great weekend in Montgomery, Alabama, after a terrible week in Boston. I was lucky to have no problems at the airport, given the tight security, and arrived in sunny Montgomery Friday afternoon. I was greeted by a wonderful display at the Renaissance Hotel: streamers of green and purple, big Mardi Gras-style mask, and the warm hospitality of the Hemophilia and Bleeding Disorders of Alabama staff. The theme: Unveiled… Our Future Revealed, a theme the HBDA will use all year long as they raise public awareness of this rare and mysterious thing called hemophilia.
Michelle Rice and Laurie Kelley
And I was surprised by a lovely and patriotic display of fireworks right outside my hotel window that night!
On Saturday morning, while the kids were organized to be bussed to the local zoo, we adults visited another kind of zoo—the world of health care reform! Our session kicked off with a full audience of about 100 people with hemophilia and their families. “Pulse on the Road” is a three-hour insurance symposium that
brings our newsletter Pulse to life.
This year we will visit six states; we’ve already been to New York for Albany Days and Colorado for the annual meeting.
Our guest speakers were Michelle Rice, public policy director at NHF, of course, and Marvin Poole, a senior reimbursement manage with Baxter Healthcare, sponsor
of this symposium.
Laurie Kelley with Vicky Jackson
Marvin opened with a review of the Affordable Care Act (ACA) which led to an explosion of questions. The audience, attentive and curious, was hungry was answers. I jotted down questions as they came:
1. Will your employer be able to deny you due to hemophilia?
a. Marvin replied no. Under the ACA, no pre-existing condition exclusions are allowed.
This is one of the beauties of the legislation!
2. Will the “navigators” (the helpers who will guide us using the new exchanges, now called marketplace, websites where we can buy insurance) be neutral? Or will they work with the payers? Whose side
are they on?
a. Michelle noted that they are not on
anyone’s side. They are trained to be neutral, and are there to help us
evaluate the cost versus the benefits of any given plan, to help us decide
which is best for us.
3. What are the essential health benefits?
a. Michelle noted that certain packages called essential health benefits (EHB) must be included in all insurance plans. These are basic services that must be covered. But… the definition of what these things are may differ! For
example, ER coverage when there is an emergency. What’s the definition of an
emergency? For Michelle it might be an ear infection as she travels a lot. But for a payer, it might be loss of life or limb!
4. Are payers going to cap insurance for premiums? I’m paying $900 a month!
a. Marvin answered that there will be a cap on copays, but premiums will be expected to rise.
5. Explain what the marketplace is.
a. Michelle replied that these are web portals (websites) created by the states that allow people to “shop” on line
for insurance plans. You can plug in your requirements and needs, and the system will bring up various plans for you to compare. These plans will be denoted by a cost-sharing scheme: Bronze, Silver, Gold, and Platinum. You can choose one of these plans based on how much you are willing to pay. For example, a Bronze plan might be 60/40; you pay 40%, with lower monthly premiums. A Platinum might be 90/10, with high premiums but lower out of pocket costs after that.
But Michelle noted that the maximum out-of-pocket (OOP) costs to us, consumers, for health insurance through the marketplace
regardless of the plan are $6,200 for an individual and $12,000 for a family. What counts toward it? Copays, coinsurance, deductibles related to EHB.
6. What about tiers? If you have a Platinum with 90/10 cost sharing, even 10% of the cost of factor is outrageous.
a. Michelle replied that our understanding is that your OOP, even with tiers, goes toward that OOP max in the marketplace.
7. If you have private insurance, can you still use the marketplace?
a. Not if you have a large employer. As of now, no.
8. What about Medicaid? What changes will happen there?
Brian Ward, president of the HBDA said Alabama is not currently managed Medicaid, but might be soon. Managed Medicaid is when it is managed by a payer like Blue Cross Blue Shield (BCBS) or Aetna, for example. It may have a PDL or formulary which lists the drugs covered by your plan (know this one, for factor!). Michelle said it is very much like a Medicaid HMO: it uses a Primary Care Physician (PCP), and in network hospitals and physicians. Coverage will be the same for services but the networks will be different.
With friend Kelly Champagne
9. Can payers reject prophy on Medicaid managed care?
a. Michelle: NHF hasn’t seen formularies yet r restricted prophy. They will restrict factor provider (meaning specialty
pharmacy). They seem to “get” prophy for kids, not so much for adults and may argue that coverage.
b. Michelle also replied that most changes in Medicaid are not related to ACA. Managed care has been with us for years, and now Medicaid is trying to use it for more groups like hemophilia. Sometimes managed care is better for us all, but the biggest problem for us all is coverage for factor.
One mom lamented, “My son uses $30,000 a month and he’s only 2 year old. I can’t have caps!” Brian then stressed: tell us your stories, your struggles, because we will then tell Michelle at NHF and NHF will can set policy.
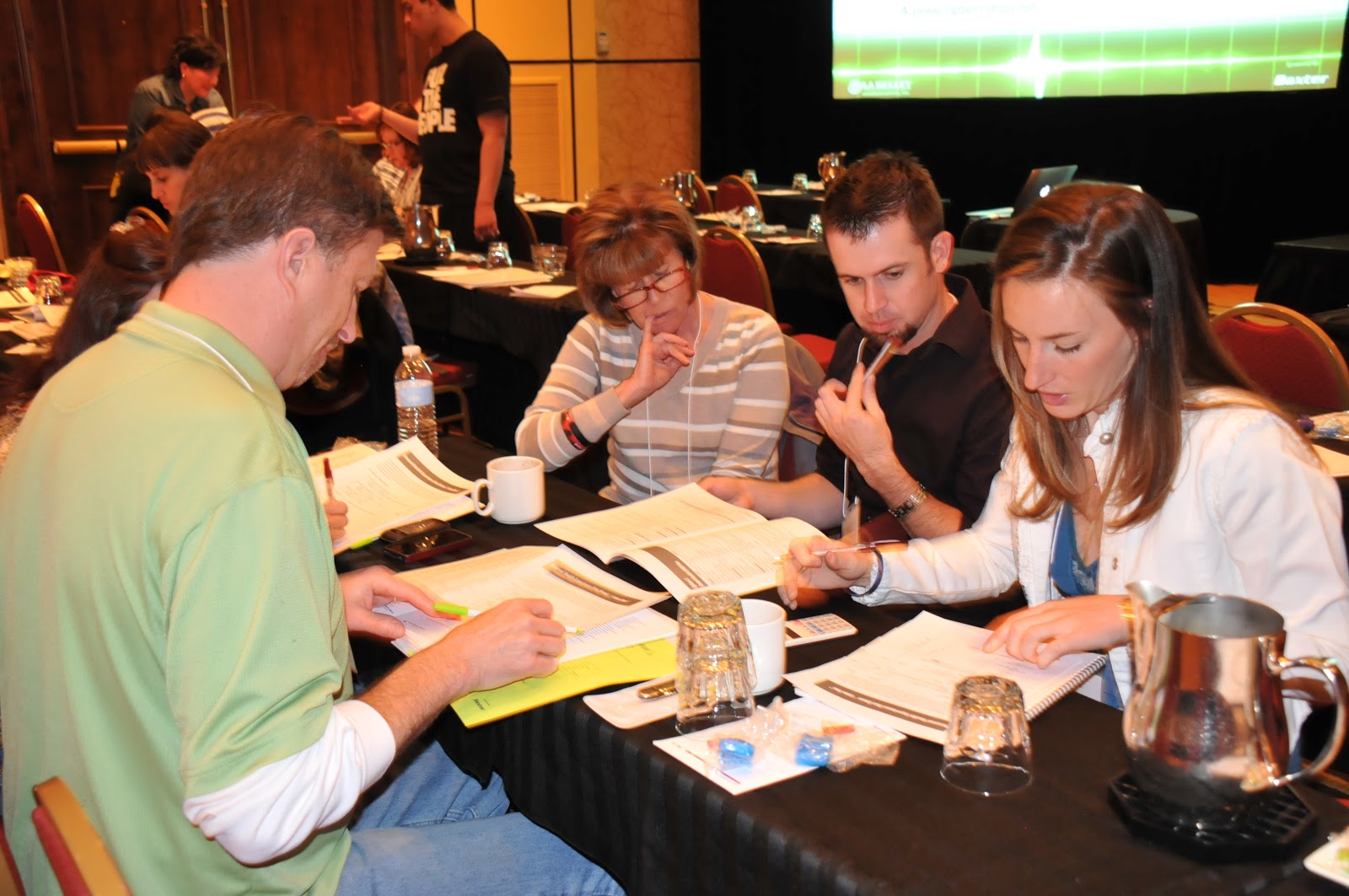
After this lively session, I then spoke for 20 minutes about the importance of being able to choose your health care plan, followed by Michelle Rice’s excellent hands-on seminar about NHF’s toolkit, which has attendees crunch through numbers
to calculate the different between two plans for “John Doe,” who must choose between two plans. Wow, the numbers were flying, and attendees quickly calculated the costs. This is a great exercise for families who feel intimidated by insurance policies and questioning charges.
Laurie with Tricia, a mom with a child with hemophilia
It was an engaging, excellent three hours, filled with inquisitive audience members (every speaker’s dream!), and much information sharing. It is a lot to absorb but family members came away with new tools, new ideas and more solidarity.
Thanks to the Hemophilia and Bleeding Disorders of Alabama for inviting us, to Vicky Jackson, executive director extraordinaire and her team, and Brian Ward, president. And to Baxter Healthcare for sponsoring Pulse on the Road and to all the companies who supported this wonderful weekend!
For more information on insurance, download Pulse on the Road for free at https://www.kelleycom.com/newsletters.html.
Great Book I Just Read
Angela’s
Ashes by Frank McCourt
Poignant, page-turning and superbly written story, based on the author’s life, of growing up impoverished in Ireland during World War II. If you’re Irish, you will especially love the historical references, phrases and cultural mind-sets, things we all heard growing up. But mostly this is a book about how a child thinks and perceives his world when he is trying to survive harsh poverty, hunger, loss of siblings, alcoholism, an absentee father and the brutal reception he receives from most adults, including those of the Catholic church. Five/five stars.
The Colorado Chapter of the National Hemophilia Foundation is flourishing under the leadership of Amy Board, executive director and her team. We had an excellent turnout for our Pulse on the Road insurance symposium yesterday, presented at the Colorado Chapter’s Educational Dayz! 2013.
Friday night started with a fun ice-breaker, dinner and then a great presentation in joint care by my friend Jeff Kallberg, a physical therapist who has hemophilia. This was followed by a carnival in the ballroom. There were lots of children and their families attending, so the whole event was kid-friendly, of course!
On Saturday, I was joined by Michelle Rice, policy director of NHF and Frank Quintieri of Baxter Healthcare to present Pulse on the Road. Frank gave an overview of the Affordable Care Act (ACA). In a quick review he stated that the ACA, passed in 2010:
Lifts lifetime & annual caps
Dependents stay on parents’ plan till age 26
Eliminates pre-existing condition exclusions
Creates “marketplaces”
Allows states to expand Medicaid eligibility
Frank explained each of these changes in detail, all of which was good news for people with chronic disorders. The audience had excellent questions in response to his talk, from how does the ACA affect the self-insured plans, to what happens when a child with hemophilia turns 26 and then doesn’t have insurance. We all agreed that this was one of our most inquisitive audiences to date!
I spoke after a break about the importance of choosing a healthcare plan: you need to know terms used by payers, where factor is charged on your plan (major medical or pharmacy?), and what are the costs versus the benefits of the plan? Beware of what is covered in–network versus out-of-network. And most of all, know when your open enrollment period is—the time when your employer chooses a new plan. We all had a great laugh when audience member Maryann called it open season; “Like deer hunting?” I replied.
Michelle Rice presented NHF’s excellent Insurance Toolkit, designed to walk you through a hypothetical patient who wants to compare two plans. It’s detailed, challenging and incredibly useful. If you can do this Toolkit, you are ready to compare plans under the ACA through the marketplaces. The audience dug right in and got to work, using the calculators we supplied. And right away people caught on that there was a trick question when it came to plugging factor costs in! Impressive!
In summary, we reiterated that:
Everyone must have health care coverage in 2014
You may need to select your coverage in a marketplace
You must read your insurance policy annually
Hats off to Amy and her team for an excellent weekend, and for being such gracious hosts for us. We’re excited to see Colorado flourishing!
No book review this time. Colorado patient Chris Bombardier, who summited Mt. Aconcagua in Argentina in February (first person with hemophilia ever to do this!) and girlfriend Jessica Carter kindly spent the day with me Sunday to take me hiking and caving. The original plan was to hike 14,000 ft Pike’s Peak but conditions were very bad—high winds and lots of snow. But we had a great day hiking the Gardens of the Gods, and later visiting the Cave of the Winds. Beautiful rock formations under ground, a mile of stunning beauty including stalactites, stalagmites, columns, cave popcorn, cave bacon and soda straws. Colorado has tremendous natural beauty: go see it if you can!
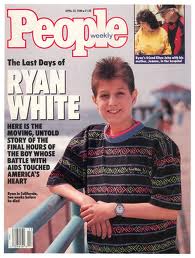
This morning my friend, Barry Haarde, and many of those on Facebook reminded me what a special day it is. The anniversary of the passing of one of the heroes of the HIV/hemophilia community, Ryan White.
I recently met someone my age who had never heard of him. It seems hard to believe, given that he was a pioneer in advocacy for the rights of those with HIV, at such a tender age. And HIV in the 1980s was paramount to the plague, the Black Death, sweeping the country and causing people to react with fear, superstition and discrimination towards those who contracted HIV.
Ryan was born December 6,1971, to Jeanne White, in Kokomo, Indiana, who learned three days later that her baby had hemophilia. Treatment then consisted of factor concentrate injections which were not pasteurized or treated to remove viruses. Shortly after surgery on his left lung in 1984, doctors informed Jeanne that Ryan had contracted HIV. At age 13, Ryan was given six months to live.
What we didn’t know then and what we know now staggers the imagination. No one could have made up a sci-fi story as incredible as a microscopic virus infecting the entire nation’s blood supply and leading to the deaths of 10,000 with hemophilia. Ryan was one of them, and one of the most famous. Why?
His fame stemmed from how he handled discrimination in the Indiana school system, which would not allow him to attend classes. Ignorance about the disease caused mass panic and hate crimes. Ryan was shunned, harassed; one night a bullet was even fired into his home.
Ryan and his mother took the school discrimination case to court. Eventually, Ryan won. He was allowed to come back to school. But, people’s minds didn’t change so quickly or with the court decree. Ryan continued to face harassment by schoolmates, and parents pulled their children out of school. Ryan faced it all with characteristic grace, dignity and acceptance.
Ryan eventually found a school that welcomed him in Cicero, Indiana: Hamilton Heights High School. He thrived there.
His story of courage found its way to the media, and Ryan became a celebrity. A made-for-TV, a biography, many television spots…. and even friendships with Elton John and Michael Jackson. Ryan was hemophilia’s earliest advocate: on March 3, 1988, Ryan spoke before the national commission on AIDS, about hemophilia, HIV, discrimination. It’s fair to say this child–a suffering child–changed the way everyone viewed HIV. He was a pioneer, a role model, and transformational leader.
He died on April 8, 1990, Palm Sunday, surrounded by Jeanne, his sister Andrea, his grandparents and his friend, Elton John. Jeanne remains fairly active in the hemophilia community and attends various events to remind us all of the importance of advocacy. Ryan’s impact goes far beyond his short time on earth, and he will eternally be remembered as a compassionate child who suffered, transformed his suffering into a mission for a greater cause, and left a lasting legacy so that others could avoid the discrimination he endured. His life is a blueprint of hope and courage in the face of alienation and pain, like so many others in our very special community.
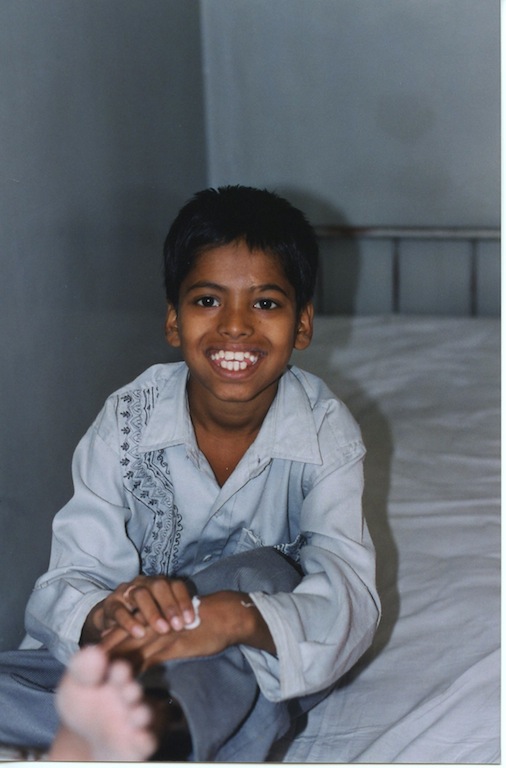
While we celebrated our own Washington Days at the end of February, and have been observing March as official Hemophilia Awareness Month, India has long been a leader in hemophilia advocacy. With a projected population of over 100,000 people with hemophilia, and only about 15,000 registered, people with hemophilia suffer and even die regularly in India. India has been lobbying its government for years, and finally the efforts are paying off, despite competition for attention from infectious disease groups, high profile crime, and politics. It’s a miracle hemophilia is noticed at all, unless you meet the people behind the advocacy. I’ve been able
to work with them via Project SHARE and Save One Life and they are smart, savvy and know how to get things done.
But progress is slow. Below is a recent article about hemophilia care in the state of Maharashtra.
“Despite promises, 3,000 hemophiliacs in state await medicines,” by Ananya Banerjee
Posted online: Mon Mar 04 2013, 05:25 hrs
Months after the Maharashtra government told the Bombay High Court that it would provide free medicines to hemophilia patients; the 3,000 registered hemophiliacs in the state are still awaiting the clotting factors that are essential to any person suffering from the disease. Hemophilia is a genetic disorder, which impairs the body’s ability to clot blood, thus increasing the possibility of the patient bleeding to death.
Currently, the hematology center at KEM Hospital gets the bulk of hemophilia patients, while a handful go to the other civic-run Nair and Sion hospitals. The factors at KEM are purchased by the Hemophilia Federation of India and disbursed at the centre.
“The government has made several promises to support hemophilia patients, but next to nothing has materialized. The disease is under-reported, especially in the rural areas. Many die due to lack of
access to treatment. Other states such as Assam, Uttar Pradesh and Madhya Pradesh are giving free factors to patients,” said Dr Kanjaksha Ghosh, director of the National Institute of Hematology.
Replacement of the factors VIII or IX, essential for preventing continuous bleeding, cost a patient a minimum of Rs 9,000 ($165) at one time. A severe hemophiliac may require as many as 1,50,000 units of
factor per year.
“The government has not made any move on providing free factors to us. We have earmarked Rs 50,000 from the hospital budget to treat haemophilia patients. This is, however, not enough,” said Dr Sandhya
Kamat, dean of KEM Hospital.
While the state currently has 3,000 recognized and registered hemophilia patients and the city has 1,500.
The Haemophilia Society, Mumbai chapter, filed a PIL in the Bombay High Court last year, demanding better treatment mechanism for hemophiliacs and make treatment affordable and accessible. The matter is still pending in court.
Meanwhile, the state, which launched its ambitious healthcare scheme, Rajeev Gandhi Jeevandayee Arogya Yojana (RGJAY), last year, has not managed to treat any hemophilia patient even after completing over 25,000 surgeries.
“RGJAY is not the appropriate model for hemophilia treatment. For every infusion, the frequency of which may vary, a patient has to get admitted to the hospital and wait for factors before the treatment can happen. This is a waste of resources and the money, which the beneficiary is entitled to,” said Paresh Parmar, secretary of the Haemophilia Society, Mumbai chapter.
Ashok Verma, founder of Hemophilia Federation (India)
“What is required is setting up of centers across the city and the state with trained staff and availability of clotting factors. While the government has been assuring us these for a long time, nothing yet has been done,” Parmar said.
I’ve been to KEM Hospital and know the Haemophilia Society, Mumbai Chapter. They are miracle workers, helping hemophilia patients with so few resources. Project SHARE is proud to continue to offer factor when possible, while the local chapters and the national Hemophilia Federation (India)
continues to lobby the government for support. We wish them continued success.
HemaBlog Archives
Categories
Download Now
Would you like to be added to our email list to continue to recieve future editions of PEN in PDF format?
LA Kelley Communications - You are leaving our site
You have clicked on one of our advertiser’s links. Our provision of a link to
any other website or location is for your convenience and does not signify
our endorsement of such other website or location or its contents.
















 Ryan eventually found a school that welcomed him in Cicero, Indiana: Hamilton Heights High School. He thrived there.
Ryan eventually found a school that welcomed him in Cicero, Indiana: Hamilton Heights High School. He thrived there.