It’s Halloween season again, and always a fun time to look at the lore of blood-drinking creatures, known as hematophages. In the past we’ve looked at the relationship between vampires and hemophilia—some studies even thinking the lore of vampires may be started with cases of hemophilia, unknown at the time. What are other blood-drinking creatures from different cultures? I found this summary on the internet:
The Chupacabra, from Latin America, which drinks goat blood. It’s a bear-like creature with spines on its back. This myth dates back only to 1995, when a farmer in Puerto Rico found dozens of his sheep drained of their blood with small circular incisions on their bodies.
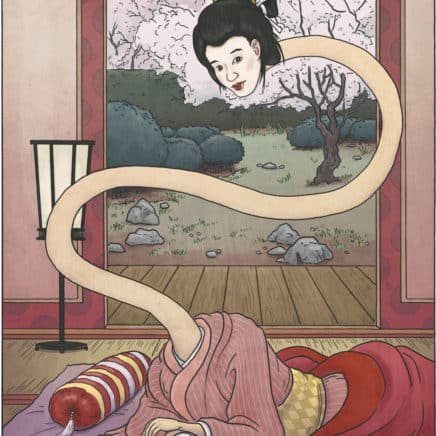
A Rokurokubi
The Baobhan Sith, a fairy in Scottish lore that drinks human blood, and usually appears as a beautiful young woman wearing a long green dress that conceals the deer hooves she has instead of feet.
Rokurokubi is a kind of Japanese apparition, whose name means “pulley neck.” By day these are regular women. By night, their bodies sleep, while their necks stretch to amazing lengths and roam around. There are two types; the others’ heads come off and fly about, and feast on blood.
Lamashtu is a Mesopotamian goddess/demoness that drank the blood of children. She is depicted as a mythological hybrid, with a hairy body, a lion’s head with donkey’s teeth and ears, long fingers and fingernails, and the feet of a bird with sharp talons.
Jubokko, another Japanese apparition, was once a normal tree that eventually absorbed the blood from battlefields, and became alive as a spirit. Afterward, the tree only craved human blood. When someone passed by, the tree grabbed them with its long branches, pierced their skin, and sucked out their blood.
Yara-ma-yha-who, a creature from Australian Aborginal mythology. The creature looks like a red amphibian- man with a very big head, large mouth with no teeth and octopus-like suckers on the ends of its hands and feet. It lives in fig trees and, like the Jubokko, waits for an unsuspecting traveler to rest in its shade. The creature ambushes the traveler, using its suckers to drain his blood. Then, it swallows the traveler, and goes to sleep. Upon waking, it regurgitates the victim, who is alive, but shorter, and who in time becomes a Yara-ma-yha-who.
And finally, we return to vampires, the kind we are more familiar with, but from China. A jiangshi is known as a hopping vampire, created from a corpse when a cat jumps over it! It moves about by hopping with its arms outstretched, kind of like Frankenstein’s monster. It kills living creatures to absorb their qi, or life force. Like the vampire folk tales we are familiar with in the west, they prowl about at night, and sleep in coffins or dark places such as caves in the daytime.
All cultures seem to love a good scary story, don’t they? And blood seems to always be a component of scary tales—I had a few of my own when raising a child with hemophilia!
It’s that time of the year again… Open Enrollment, when you can change your health insurance policy or plan. But you can’t change unless you know what your needs are, and can calculate what your budget is and what expenses will be. Insurance is frustrating, it’s daunting, and with a bleeding disorder, it’s expensive.
But I just saw this on Facebook, which made me happy for two reasons: 1) a licensed insurance broker can help you get started for free, and 2) he’s a wonderful person I’ve known for a long time.
Meet Alexander Ell!
For over 10 years, Alex has helped over one thousand clients with their insurance across multiple states and numerous insurance companies. Alex’s goal is to walk you through the process, providing non-biased advice about the best plan for your needs and goals. His website helps you learn the basics of insurance, defines the many acronyms that insurance loves to use, and has a Frequently Asked Questions section.
On Facebook, he wrote: “Hey everyone! If you hear of any friends or family that need help with their Medicare or Health Insurance, please send them my way. I’ve been a licensed insurance broker for over 10 years. My services are free and I provide non-biased advice about the best plan for their needs and goals. I’m licensed in ID, NV, OR, WA, TX, GA, and FL. If you have any questions, please reach out to me. https://capitalrealm.com”
Alex has navigated the complex healthcare system for himself as he has hemophilia. Now he’s here to do the same for you! Contact him to get started with a free consultation today.
My boyfriend Doug is such a go-getter, such a team player, that I would always tell people, You want something done? Doug’ll do it. And I volunteered him for various tasks at Save One Life, which he cheerfully accepted and did. One year I even made magnets and lapel buttons for the Save One Life team that read “Doug’ll Do It!” as a joke.
It’s no joke now. Doug did it! He cycled 3,784 miles coast to coast—from Portland, Oregon to Portland, Maine, arriving Thursday, October 5 on a grey and windy day in Maine, to dip his wheel in the Atlantic Ocean. It was an incredible feat, for someone who is 66, and only took up riding nine years ago, when he first met me. Combined, his efforts and those of our community around the country who participated in the Wheels for the World campaign, raised over $230,000 to support the mission of Save One Life, the nonprofit I founded 21 years ago. It was our biggest fundraiser ever.
Doug is inspired by Save One Life’s mission, to give direct financial support and medicine to those with bleeding disorders in developing countries. Save One Life assists over 1,200 people who live in poverty, in India, Pakistan, Nepal, Kenya and ten other countries. It offers direct sponsorship, college scholarships, microenterprise grants, camp support and millions of dollars worth of blood-clotting medicine.
But Doug was also inspired by an incredible individual: the late Barry Haarde.
Barry was an avid cyclist with hemophilia who completed six—six!—long distance tours over six years to raise money for Save One Life. From coast to coast, with his final one dubbed “Call of the Wild” from Dawson Creek, British Columbia to Anchorage, Alaska. His tours totaled over 20,000 miles and raised over $230,000 for Save One Life!
What was remarkable about his achievement was that Barry had hemophilia, HIV and a contracted knee joint… health issues that would stop most people from considering this audacious ride. But Barry was not most people…he was driven by memories of the brother and brother-in-law he lost to hemophilia and HIV, and all the friends in the community lost to HIV. In addition, he knew firsthand the pain suffered by those in developing countries who often lack access to blood-clotting medicine.
Doug met Barry twice, and both learned that they loved cycling, both worked at Hewlett Packard, and both admired the work of Save One Life. Doug was in awe of Barry. Barry passed away in 2018, and no one since has dared to fill his cycling shoes. But Doug’ll do it! And he did. I’m so proud of Doug: the time he invested in training all year, the time spent away from me and home, his dedication and discipline, and his accomplishment.
Thanks to all who donated to this cause, thanks to our major sponsors, Sanofi and CVS, and for all the prayers. Through the Rockies, the cornfields, the highways and hills, he was safe and is now home. And Save One Life continues on, to help the needy.
Yesterday was a celebration of his accomplishment and a surprise announcement! We have a new volunteer for next year! James’ll do it! James is from Texas and was a friend of Barry’s. So the torch has been passed and we wish James much success in 2024!
It’s normal for anyone to be concerned at the thought of a child with hemophilia in the classroom, but it can especially worry the teacher, who bears responsibility for the students. Even if the teacher has some knowledge or experience, no two children with hemophilia are alike. Chances are, yours will be the first child with hemophilia that his teacher has met.
A group of seven multi-ethnic elementary school children, 7 to 9 years old, standing outside a building waiting to board a yellow school bus.
Many teachers have taught children with special needs, and they may be completely comfortable with your child. But for others, your first meeting may only temporarily relieve worries. A teacher could develop new concerns when left alone with your child for the day. Afraid of injuries, fearing the sight of blood, and anxious about being held responsible, a worried teacher might—without meaning to—show negative behaviors like overprotection, singling out, denial, and overreaction.
Overprotection
Fearing injuries, a teacher may want to exclude your child from some activities. Provide a list of activities that are safe for your child: using scissors, playing on the concrete or asphalt surface, using playground equipment, jumping rope, playing kickball and tag. If you want to forbid a specific activity—like hanging by his arms from the jungle gym after a forearm or shoulder bleed—write a note or email his classroom and physical education teachers. Ask them to find creative ways to include your child in an activity, even when a bleed sidelines him. He could be the assistant “coach” or scorekeeper, for example.
Singling Out
Your child’s teacher may accidentally single him out by announcing to the class that he has a blood disorder. The teacher may constantly remind other children not to hit your child. The phrase “Now, everyone except . . .” calls attention to your child. Most children dislike this kind of attention. Too much attention, especially when it sets a child apart from classmates, can produce resentment. Your child could be rejected or teased by classmates.
If your child must avoid a particular activity (with your approval), teachers should arrange a face-saving, tactful way to exclude him—one that doesn’t attack or shame him or draw attention to his disorder.
Denial
On most days, your child can participate in all activities and show no signs of bleeding. On other days, your child must be excused from certain activities when he is recovering from an injury or bleed. Outwardly, he appears fine, and his teacher may not recognize the need for rest. It’s even harder for the physical education teacher, who often hears a long list of illnesses and complaints from children who simply don’t want to run laps or climb ropes. Remember to stress that all teachers should trust your child’s judgment about a bleed or his recovery, with or without notes from home.3
Overreaction
Most teachers model emotionally mature behavior in the classroom, but some may gush “ooh” and “aah” over a child’s bruises and swellings, or exclaim, “Poor boy!” They may have good intentions, but this puts a spotlight on your child. He feels different from his classmates, and may develop negative feelings about hemophilia. Injuries and bleeds should be handled calmly and competently, with concern but with minimal fuss.
Teachers provide information about our children’s development. Teachers tell us how our children are adjusting to school. They can alert us to signs of depression, like withdrawal or slipping grades, which may indicate poor self-image or adjustment. They can tell us whether our children are interacting well with others or being bullied. They notice if our children are afraid to take risks.
Communication, trust, and respect between parent and teacher are key building blocks of a positive student–teacher relationship. Keep communication channels open by scheduling periodic meetings to answer school personnel questions. Consider becoming involved in school activities like parent–teacher groups. Volunteer at your child’s school. Attend open house events or chaperone a field trip, and model how you handle your child and his hemophilia. Sign up for your school’s online parent portal. Keep his teacher up-to-date with events at home; for example, a traumatic bleed while on vacation, the impending birth of a sibling, or anything that might cause stress and lead to a bleed or might affect school participation and attitude. Get involved with your child’s school experience to show your positive attitude and act as a role model.
Excerpted from Raising a Child with Hemophilia, 2023 Coming soon!
A group of four multi-ethnic elementary school children, 7 to 9 years old, getting off a school bus. They are in a hurry, running as they step out of the doorway.
From ages six to twelve, your child develops from childhood to the brink of adolescence. This is a time of expansive physical and emotional growth and tremendous learning. Your child has a firm foothold on the path to independence. You want him to become independent, and you’re proud and happy to see him blossom. Yet you may have mixed feelings as you watch your child enter school for the first time.
Just as life settles down, and you feel competent and comfortable with hemophilia, the rest of the world will now meet your child with hemophilia. The child you loved, nurtured, and protected is now among other children and teachers who know little about his condition, in an environment beyond your supervision. It’s normal to feel anxious!
Your child may be anxious, too. School is his first venture into the “real” world. He will make independent decisions about his behavior, and he’ll take on more responsibility. He will interact with other children and make friends. With solid self-esteem, knowledge about hemophilia, and your unconditional love, your child will shine during these formative years!
FROM PRESCHOOL TO FIRST GRADE
It’s rare these days to find a child who spent his first five years at home full time, and this includes children with hemophilia. If your child has attended daycare, preschool, or pre-K, you may feel confident handling primary school issues related to hemophilia.
Regardless of how your child spent his preschool years, attending kindergarten means that he will be mainstreamed in a classroom. He’ll be supervised with up to 25 or more youngsters. Never has your child been so free to test his limits. You may worry constantly whether anyone will notice that he bumped his head or hurt his knee. You’ll wonder if your child is responsible enough to report that he has a bleed.
By the time he reaches first grade, your child may be graded or compared to others. He will begin to learn about his world through his class curriculum, and he’ll be expected to keep up with his peers. He may start having homework. If he misses school or homework assignments because of hemophilia—an elbow or wrist bleed, for example—he may feel anxious. Fortunately, given current medical care and prophylaxis, bleeds should rarely result in school absences.
Making sure your child is happy, confident, and healthy is a team effort now involving you, your child, and school personnel. What should you tell the school personnel? How can you promote the best understanding of this rare disorder? How will you explain hemophilia to your child’s classmates?
TELLING SCHOOL PERSONNEL
Put yourself in a teacher’s place: You have a classroom full of small children, all with differing backgrounds, personalities, energy levels, abilities, and challenges. Your job is to instruct them, manage them, account for individual differences, foster cooperation, evaluate their development, and have fun—for six hours every day! As the school year begins, you learn that one of your students is a wonderful child with a rare bleeding disorder. What now?
For the inexperienced, hemophilia may create images of intense bleeding, emergencies, and chaos. School personnel wonder: Can he use scissors? Can he play at recess? Is he as intelligent as the others? How can I watch him and the other children, too? What happens when he gets hurt? Will he bleed excessively?
Remember how much better you felt as a parent when you armed yourself with knowledge? Your child’s teachers will, too. But how do you begin?
Contact your HTC for assistance when meeting with school staff. The HTC staff will advise you, or may even come to school with you.
Order resources from HFA or NBDF to leave with school personnel.
Arrange a first meeting with school personnel before school starts.
Your first meeting should include the following:
Your child’s classroom teachers or head teacher (in lower grades)
Assistant teachers or teacher’s aide, if any
Principal, vice principal, or counselor
Physical education teacher
School nurse, school district nurse (if no nurse at school), health aide, or health clerk
Ask your HTC nurse or home health nurse to attend. This lends credibility and a professional perspective. Your HTC representative may also want to meet with school personnel privately to answer any questions they’re hesitant to ask in front of you.
Your child doesn’t need to be at this first meeting, although he should be told about it. Ask your child if he’d like to attend. He can practice taking personal responsibility for his health by speaking directly to school personnel about his abilities and any limitations.
Give school personnel some materials to read, but don’t overload them with information. Audiences usually remember only three main points of any meeting, so choose which three you want to emphasize. Your first meeting’s agenda should be simple and focused on handling hemophilia in school:
Explain hemophilia, and dispel myths.
Describe the symptoms of a bleed: swelling, limping, favoring a limb.
Describe the types of bleeds your child is likely to have.
Explain the different severity levels, and share your child’s level.
Describe your child’s specific limitations and abilities: he can play at recess; he can’t be hit in the chest with a kickball.
Emphasize that your child should be treated normally.
Supply your contact phone numbers.
Reassure everyone that they will not have to learn how to infuse.
Ask that factor be stored in the nurse’s office. (This may not be possible in private schools without a nurse.)
Provide emergency numbers and instructions in case you can’t be reached: HTC, hematologist, local pediatrician.
Reassure school personnel that they can treat your child normally, and they can believe him when he says he needs treatment. They should never single him out, announce that he has hemophilia, or make an issue of his medical ID bracelet or his bruises. They should take normal precautions and follow normal safety practices. Remind them also to follow standard first aid procedures for most injuries. This treatment should not be delayed while they try to notify you.
Later in the school year, you can meet again. School personnel will have more questions and may be more comfortable and eager to learn, as you once were.