“I speak of Africa… “
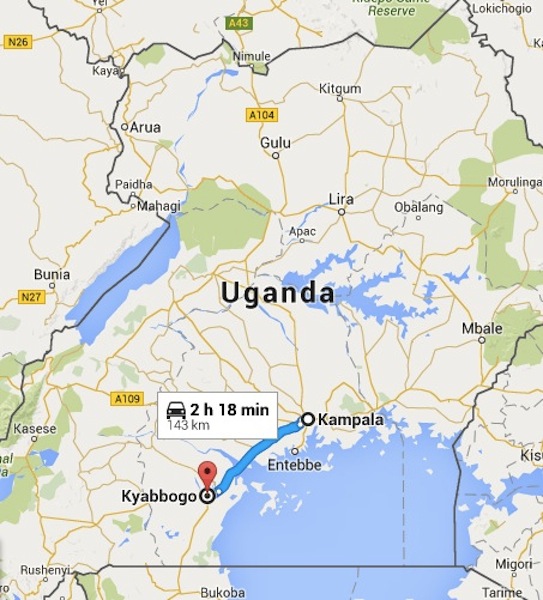 |
| By our calculations–5 hours! |
I speak of Africa and golden joys—William
Shakespeare from Henry IV, Part II c. 1597
 |
| Kampala farmer’s market |
Last Saturday, April 23, Agnes Kisakye, the executive secretary of HFU, arrived in a hired van at 7:30 at my hotel, the Sheraton
Kampala, which is perched atop one of Kampala’s seven hills. We first stopped at the city square
market for bananas for breakfast. I didn’t get out of the van, but we were
swallowed up in a swarm of Ugandans, all busy shopping, negotiating prices,
filling plastic bags with fruit. A hive of frantic activity. The bananas–called kabaragara--were
small and sweet and I devoured three. The day was cool with blue skies. We were
ready for a long road trip, south of Kampala.
 |
| Carrying banana leaves |
 |
| Scenes as we leave Kampala |
It turned out to be way longer that we thought. A
three-hour trip became 5+ hours trying to find this one family in Kyabbogo. At
least we had a very comfortable van and Agnes is a great travel companion. She
is only 29, but very mature, socially conscientious and dedicated. She’s a registered social worker, and I was quite
impressed by her. I wish I could have tape-recorded the things she said; so much wisdom, though I knew many of these things because it’s the same in so many
countries. Her brother Joseph, now an MP (member of parliament), is the person who contacted me back in 2008 requesting help.
 |
| Tea plantations |
[In fact, Agnes reminded me that I was the first to help Uganda. In 2008 an Indian working in
Uganda who had a child with hemophilia, Satish Pillai, emailed me about setting up a
foundation, and getting factor for his son. We worked together through email only, and he did all the groundwork in establishing the HFU. Satish later had to return to Mumbai, India but
appointed Joseph Ssewungu, a headteacher and father of a child with hemophilia, to replace him. Joseph and I had a
few emails back and forth, and in one he mentioned he had read my book, Raising
a Child with Hemophilia. I found that amazing. But eventually things quieted, and other countries in need diverted my
attention.
 |
| Beauty of Uganda |
We stopped en route to buy groceries for the families. Though it
was just a little street market store, we got carried away and spend $120.
Agnes seemed aghast at how freely I spent money; she was hesitant to suggest
anything because she didn’t want to take what she thought was all my money. We
bought rice, sugar, salt, Coca-Cola, cookies, lollipops, Vaseline (“For their
skin,” Agnes said), soap—lots of soap—tea, loaves of bread, and cooking oil.
Christian. We agreed that this work was our calling in life, and nothing could
stop us from helping the poor and suffering. I asked her when she knew she wanted to be
a social worker.
recalled, “since I was young. I wasn’t sure exactly what I would do. But I
loved it, the idea that I would make a difference in someone’s life. I always
wanted to start an organization. I said to my friend one day, ‘You and I will
start an organization to help people’.”
It hasn’t been easy trying to get the Haemophilia Foundation of Uganda
off the ground. “Being a volunteer is difficult. Some people show interest and
start to help us, but later they quit. I used to work as a volunteer for an
NGO, for HIV/AIDS education.” But when Satish left, she felt compelled to help
her brother full time. Now she volunteers full time, Monday through Friday and
many a weekend, to run the HFU. There are days when she stays at the Mulago
Hospital all day and into the evening—meeting with doctors and staff, and
counseling patients.
a right, and the road deteriorated from paved to dirt roads, rowdy and
unpredictable. We had stopped many times along the way, to ask locals on the
side of the road where we were going. The frequent stops allowed me to drink in
the fleeting scenery: the dusty, red clay roads that branched off from the
highway and paved roads, forming a network like blood vessels throughout the
country. Everyone seemed to move at the same pace, languid, at ease. There are no beggars and everyone works. Down one alley, a small child
in shorts and plastic sandals lugs a huge blue plastic container with water and
disappears into a slum. Roadside shops sit shoulder to shoulder: one sells
tires, one sells headboards for a bed, unvarnished and raw, another sells colorful
clothes and markets them on stark white mannequins, oddly out of place. Some
young men wearing dusty clothes and a few teen girls in worn and damaged dresses—obviously
donated (one is a shiny party outfit; one looks like a Halloween Tinkerbell
costume; another is a tight club dress) wait patiently at a pump while a young
man furiously wields the handle to draw water from the community well; a small wooden
cart belches thick smoke from the meat cooking on it, filling the air with a delicious
smell of beef, and I realize I am suddenly hungry; plump women, wearing
colorful wraps around their waist and patterned turbans to protect their hair
from the dust, balance fruit and vegetables on their head to sell or to bring
home; three little children, the dust turning the color of their deep brown
skin to chalk, dance in rhythm to the music pulsating from a radio in front of
a store while an adult eggs them on. Everyone is barefoot, or at most
wearing just sandals or plastic flip-flops.
if they are not too shy, they break into beaming smiles and wave. It’s
encouraged to wave back, and I try to keep the window down when we ask for
directions so I can wave. “Muzungu!”
they shout sometimes, their word for anyone not from Uganda, though mostly it
refers to white people. It’s not a slur; it’s just their word, much like when
the children of Haiti shouted “Blanc!” (White!) when they saw me, and tried to
touch my white skin.
gives way to hard red clay, with shoulders that sag, and the van rocks back
and forth with the unevenness. The rains and traffic have created deep ruts. We
roll up the windows as the van’s tires churn the clay to powder. Now the roadside stands have disappeared and only solitary homes are
spied through the thick vegetation. The homes for the most part are nice for
rural homes. Mud poured into a wood frame, and hardened, with a thatched roof,
or brick, made by hand, with a corrugated steel roof. Everything is cinnamon red.
Red dirt road, red brick homes, red-rusted steel roofs. Red and green are the
colors of Uganda.
with slums, poor hygiene, noise, pollution, alcohol, crowding, waste—but access
to hospitals and health care. There are megaslums, which defy the imagination,
where residents live like ants in an unhealthy and often dangerous colony. And
there is rural poverty, with lush vegetation, farm lands, rich soil,
fresh air, room to grow—but a lack of transportation, customers, and most of
all, lack of health care. Still, the scenery is beautiful, even if poor.
Agnes says, “That’s witchcraft.” Noting my raised eyebrows, she continued.
“Witchcraft is still practiced here, especially in rural areas. That would be a
witchdoctor’s place to meet with families. He will diagnose someone, and then
offer a remedy. It is so crazy! He might say, ‘Take the fingernail clippings of
your child with hemophilia, of the parents, of the relatives. Now go throw
those in the river. The river will carry them away and with it, the disease. Your
child will be cured.’ Or he may take some backcloth and banana leaves and wrap
up some part of the person—their hair, for example—and say now the disease is
buried.”
witchdoctor will first do a bit of research. “He checks with other people who
work with him, to learn more about the patient. What are their symptoms? Who is
sick? Who has been sick in the family? Then when the family goes to see him, he
will say, ‘It is your child that is sick?’ Yes! ‘He bleeds a lot?’ Yes! So it
looks to the family like he is magical and knows everything.”
 |
| The Kajimbo family: four boys with hemophilia |
Going to a witchdoctor sounds quaint, but it is anything
but cheap. In a country where the average annual salary is $500, and an
educated physician earns about $200 a month, a witchdoctor can charge anywhere
from $100 to $300—a session! This is the power of culture, traditional beliefs
and desperation. Health clinics are hard to find and far away. Rural families
become victim to their limited education, isolation, and the charisma of the
witchdoctors. “There are no government policies or laws regarding witchdoctors,”
Agnes adds.
destination: a vermilion brick-and-mortar home with a spacious front yard of
dirt, and surrounded out back by farming fields. This is where the Kajimbo
family lives. We unfolded ourselves out of the van and stretched, smiling at
the children who gathered in curiosity. The sun warmed our visit. We decided
first to get acquainted, and then to bring in the gifts. The mother Harriett
and father Richard came out of the house first, and shook hands, he smiling
reservedly, she smiling in anticipation. The first thing I noticed was that
their clothes were remarkably clean compared to their surroundings, as though
they had just changed. Harriett’s eyes sparkled, and her hair was a woven
masterpiece, plaited to perfection. Her dress was bright blue and white. Richard
wore a comfortable blue polo shirt and khaki pants. They were in great contrast
to the children, who were dressed in stained and torn clothes, and who went
barefoot, and had dirty face and hands. It was incongruent.
 |
| Laurie Kelley with baby Joel |
Still, the children seemed happy and at ease, and
deeply curious. We entered their home. There was no where for the family to
sit, so they congregated on a rug covering the packed earthen floor.
The baby, Joel, was fat and happy, and I was thrilled to take him, diaperless—always
a calculated risk—into my arms, and jiggle him on my knee. Agnes and I were
given the one bench in the welcoming room. Each child came to us one at a time,
and reached out to shake hands while bending deeply down on their knees; this
is a sign of respect for elders, and not easy to do for children with joint
deformities.
| Inside the red brick home: earthen floors |
Introductions: Six children, four with
hemophilia. Bad odds. January, age 15; Emmanuel, age 13; Richard, age 9; and
Ronald, age 5. January smiled but looked a bit stunned; Emmanuel had a ready,
warm, friendly smile, as if he had been expecting us at long last; Richard
conjured a mischievous smile, which made you wonder what he was thinking; and
Ronald tightened his lips at us, refusing to surrender any hospitality. But my,
were they all beautiful children. A sister sidled in through the raggedy
curtain that separated the welcoming room from the other five rooms. Josephine
seemed shy but wanted desperately to make friends with us.
laughing in no time. A pod of neighborhood children plugged the doorway,
leaning in, eyes wide open in astonishment. The driver had brought some bags
over by now, and we handed out lollipops first—no barriers were left after
that. The children saw at once that they came first. There were plenty to share
with the neighborhood children, which no doubt boosted the reputation of the
Kajimbo family. But Ronald still did not smile.
 |
| Ronald |
 |
| Emmanuel |
Agnes explained Save One Life to them, and also
that I was a mother of a child with hemophilia. This tidbit also breaks
down barriers instantly. Harriett looked at me with widened eyes now. After the
overview, we did the enrollment forms, starting with January. The enrollment
was easy as there wasn’t much information, and all of it was the same for all
four kids. They all missed an entire term (out of three annually) last year due
to bleeds. School is five miles away, and they often cannot walk the distance. They
can’t afford transportation to take them to school. When they do go to school,
they sometimes get “caned,” beaten with a reed or stick for infractions. This
is old-school British and still acceptable here. January goes to school with
8-year-olds in primary 3, because he is so far behind. This embarrasses him. He
gets no treatment; Mulago Hospital in Kampala is five hours away and requires a
motorbike ride on the rough, unfinished road we just conquered, and then
waiting for a public bus to take to the capital. And it costs $50, while
the family’s monthly income is $15-$30.
 |
| Richard |
 |
| January |
We surveyed the house: they have no electricity,
running water, indoor toilet or plumbing, or refrigerator. The floors are
concrete or red packed soil. Cloth doors separate the six rooms and it’s
impossible to stay clean, as dust coats everything. Out back, a brick shed for
cooking, an outhouse, and one rib-showing, starved black and white dog
collapsed in the heat. All the kids—same story. What do they do when not in
school? “Digging in the garden,” which means they do chores: farming, seeding,
harvesting. Harriett is only 29, with six kids, a huge responsibility. Still,
she smiles happily as she takes Joel from me.
school, or help feed them. We share the butter, rice, sugar and supplies with
Harriett, who is overwhelmed by our generosity. We hand out toys, many of them
simple, donated toys, especially the super-heroes and plastic creatures that have sat
in a basket for two years in my basement. I finally dumped the last of them in
my duffel bag, and now, Ronald holds what looks like a silver Power
Ranger-wannabe in his hands. He is dumbfounded, then catches on, then finally….
Breaks into a huge smile. Boys just love action figures, no matter where they
are.
 |
| Emmauel’s knees; all the boys have joint damage |
photos. We photograph January’s knee, particularly his prominent scar from surgery,
before he was diagnosed. He reminds me of Mitch from Haiti, who also almost
died from surgery before being diagnosed.
with a surprise: a chicken! Agnes laughs and I hold it for a photo opp. They offer the chicken as a token of their appreciation. The poor thing had its legs
trussed up and was hung upside down, then laid on the floor, immobile. Its eyes bulging, fearful, waiting to know its fate: lunch, dinner? Were we to take it back five hours to Kampala like that? I wondered what the Sheraton staff would say if I walked in with a chicken. I had to refuse, even though
this was impolite. Agnes explained to the families that I love animals and could not bear to
see it like this. The lucky chicken was paroled and January took it back outside.
As we prepare to leave, we do a
family picture, with me holding Joel. Harriett comes out of the house, and suddenly drops to her knees before me, and
holds my hand. This is unusual for an adult, I think, and I thank her but also
encourage her to stand up.
 |
| The Kajimbo’s kitchen |
We are happy when we leave, and once back on
paved ground, we stop at a hotel for lunch, feeding the drivers as well. I don’t
each much, but enjoy a Coke immensely. Agnes and I talk about what can be done
for the family, what their daily life must be like. How much $.73 a day–the cost of a sponsorship from Save One Life, will impact their life. It might be the best thing that will ever happen to them.
 |
| Agnes Kisakye and the Kajimbo boys |
 |
| My chicken! |